Introduction:
Multiple sclerosis (MS) is a chronic neurological condition characterized by progressive inflammation and demyelination of the central nervous system. The unpredictable disease course creates a variety of barriers which prevent individuals from engaging in exercise and physical activity. Symptoms such as fatigue, a low self-efficacy, and health beliefs have all been identified as reasons why individuals with MS do not engage in physical activity1-3. Collectively, individuals with MS participate in about 33% less physical activity compared to average adults4. This conclusion is sobering in light of the risk of potential comorbidities which compound disability5.
Wellness programs incorporating self-efficacy and group exercise have demonstrated improvements in physical activity for individuals with MS6-8. To date, North Carolina has very few wellness programs for individuals with MS and other neurological conditions. Barriers for initiating such programs include staffing costs, organization, and a lack of insurance reimbursement. However, telemedicine has opened the door to a variety of innovative interventions for various populations. An online program would be easily accessible for individuals with MS and eliminate any barriers related to travel. Thus, for my capstone project, I decided to design and test out the feasibility of an online wellness program for individuals with MS.
Preparation for the Program:
Before designing the program, I researched various protocols for MS-specific wellness programs that incorporated self-efficacy or exercise. The results of this literature review can be found in an evidence table, which may be useful for therapists who are contemplating designing their own wellness program (either online or in person). In addition, I had the opportunity to co-lead the National MS Society’s Free From Falls program, an eight week educational and group exercise program for individuals with MS. This program gave me a variety of tools and ideas to include in my online program.
The Program:
I decided to create an online wellness program incorporating two MS-specific educational sessions and two group exercise sessions. I chose to implement this program on a Google+ community group which also allows up to 10 individuals to participate in an online video chat. The site is free and does not require any installation. An individual simply needs a computer, a webcam, and a gmail email account to participate (I provided instructions for those individuals who needed help in creating a gmail account). Collectively, the online Google+ community group was easy to launch. A screenshot of the online wellness program is provided:
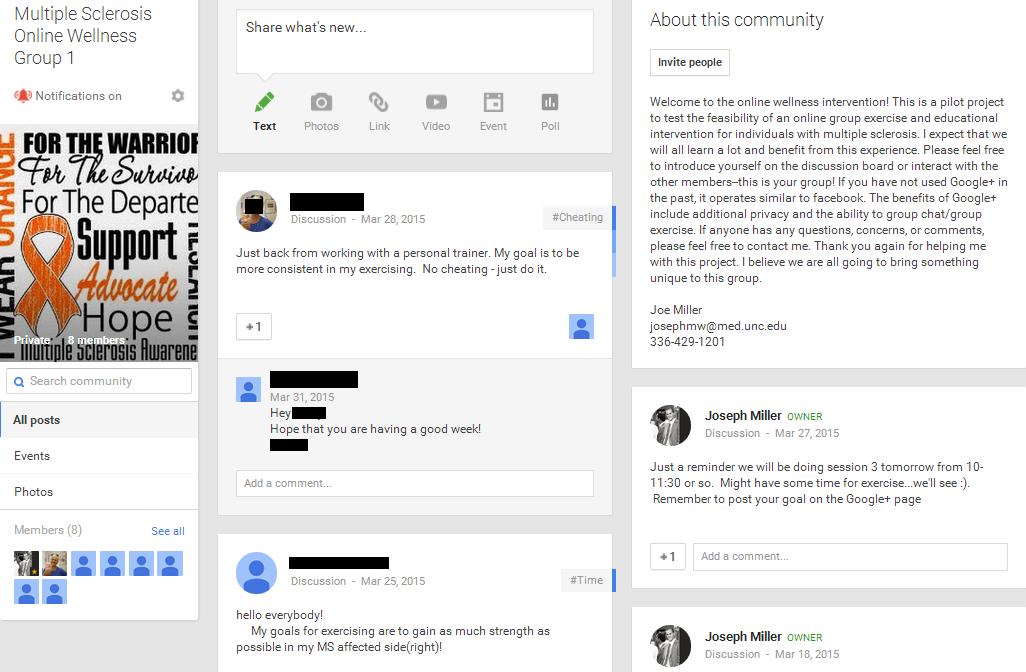 (Click on image to magnify)
(Click on image to magnify)
Five individuals with MS represented the ideal number of participants for the program: individuals would benefit from the social interaction but not feel as though they were talking over one another. Online video chat and internet-related delays affect social interaction, and I wanted individuals to feel as though they could sufficiently express themselves.
The educational sessions incorporated a variety of tools to promote physical activity and improve self-efficacy. The first educational session focused on helping individuals identify factors they could and could not control, describing the benefits of wellness and the consequences of inactivity, detailing recommended exercise guidelines for individuals with MS, and helping individuals identify meaningful goals. In particular, individuals identified a goal that they would strive for over the course of the program. A Transtheoretical Stage model was encouraged to promote an achievable and realistic change in activity. Individuals were also provided with an exercise diary to promote adherence. The second educational session focused on managing spasticity and fatigue and the role of rehab professionals in developing an exercise routine. Powerpoints from the two sessions are provided:
Education Session 1
Education Session 2
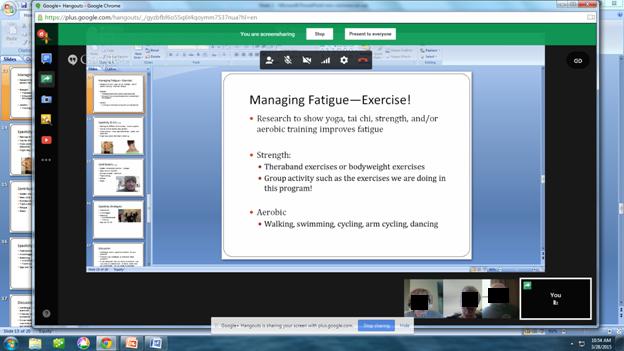
A Screenshot of an Educational Session (click on image to magnify)
Group exercise was also incorporated into the online program. Most of the exercises that were utilized in the studies from the evidence table could be performed without specialized equipment. Ten exercises from the literature were selected. Individuals were provided with an Exercise Handout which detailed the exercises along with appropriate intensity, frequency, and duration.
Outcomes
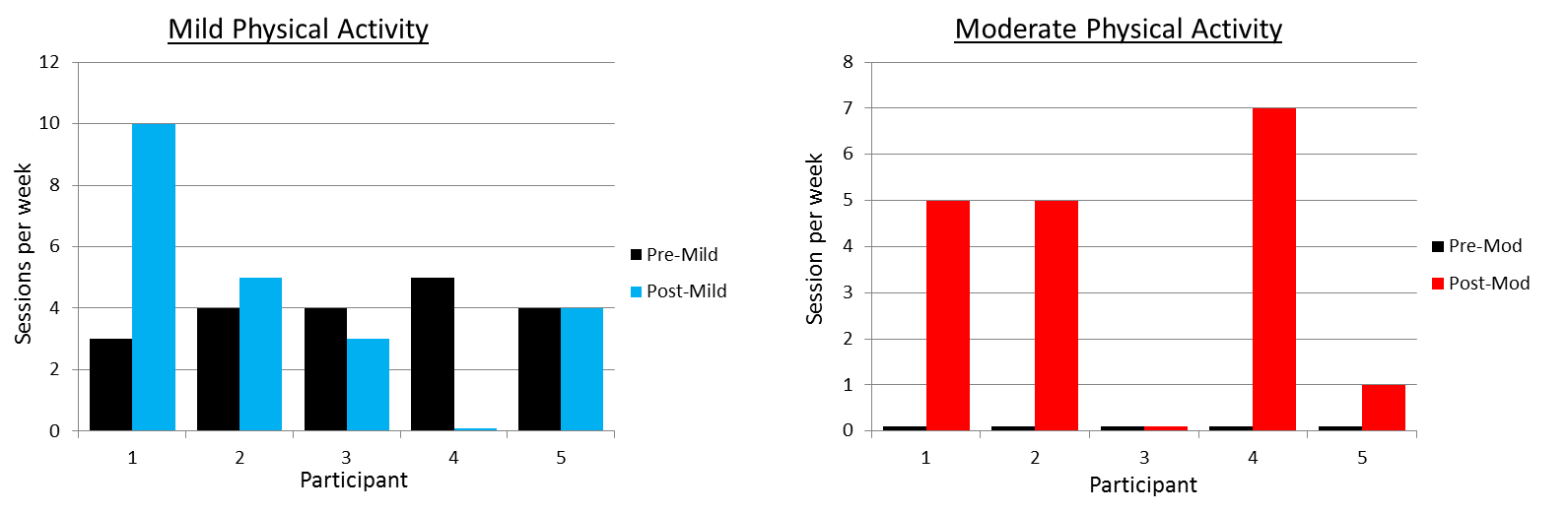
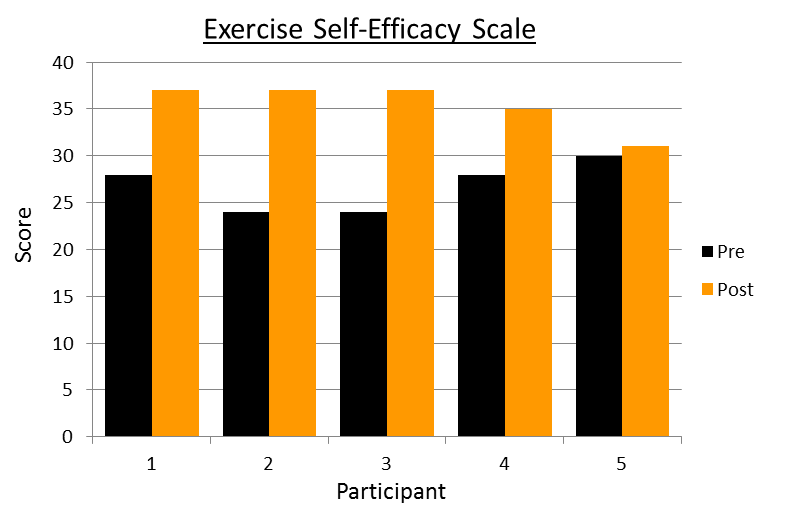
Several outcome measures were provided to the participants at the beginning and end of the program. The self-reported Patient-Determined Disease Steps scale was provided to quantify disease severity. Four out of five individuals had moderate MS (requiring at least unilateral assistance while walking 25 feet), and one individual had mild MS. The Godin Leisure-Time Exercise Questionnaire provided an estimate of the average weekly physical activity. At the beginning of the program, most individuals were participating in 4-5 sessions of mild exercise (yoga, easy walking, etc.). The SCI Exercise Self Efficacy Scale was also assessed. This outcome measures an individual’s confidence in exercising despite various circumstances or barriers. On average, individuals reported that they had moderate confidence that they could keep exercising despite various barriers.
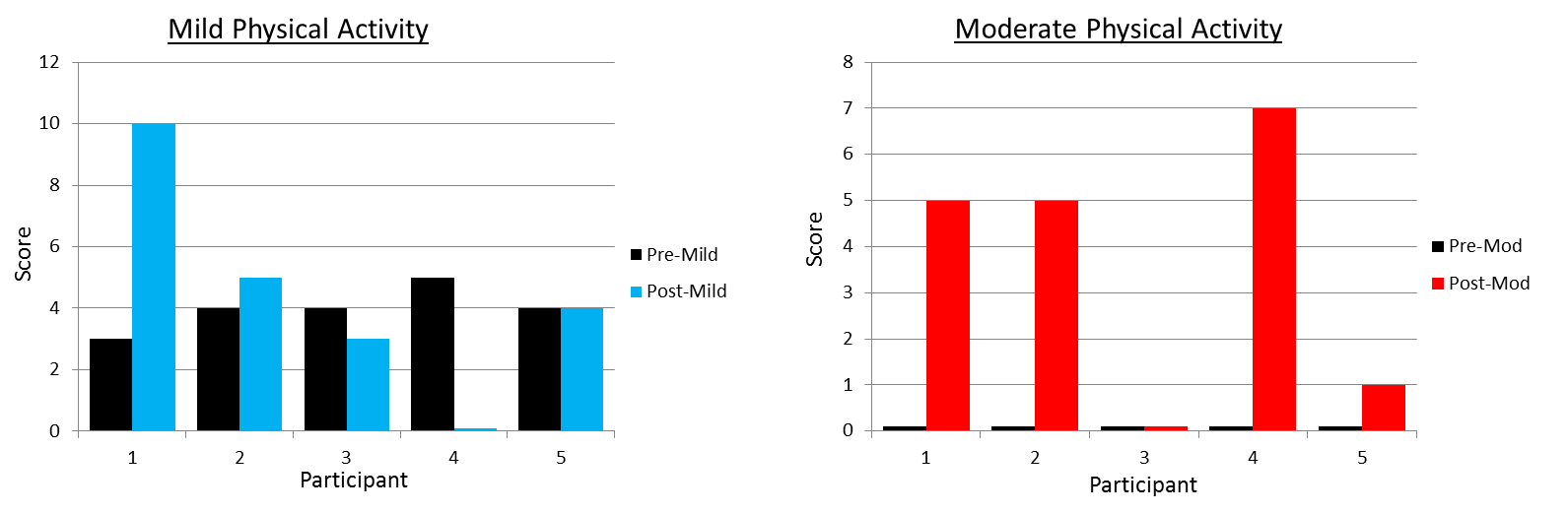
The Godin and SCI Exercise Self-Efficacy Scale were reassessed at the end of the program. 4/5 individuals either increased the amount of physical activity they were performing each week or increased the intensity of their physical activity (i.e. performing more moderate-level physical activity). The average improvement for mild and moderate physical activity was 0.4 and 3.6 sessions/week respectively:
{kind=link}
Every participant improved their exercise self-efficacy scores. The average scores improved from 26.8 to 35.4 during the program, an improvement of 8.6 points:
Evaluation:
I created an evaluation for participants to complete at the end of the program. Most patients agreed or strongly agreed that the program was easy to access and set up, the educational materials and exercise were appropriate, and they would rather exercise online instead of having to drive somewhere to exercise. One participant with mild MS did not find the exercises challenging and would rather exercise in person instead of use an online program. Most individuals reported goal-setting as the main tool which helped them increase their physical activity. Collectively, individuals reported that they enjoyed the comradery among the group and hearing recommendations from the other participants. One participant reported that she enjoyed having the opportunity to share her fears and “get a good laugh when appropriate.” A few individuals reported issues with the technology: individuals were occasionally disconnected from the sessions, people were occasionally difficult to hear, and two participants experienced lag times with conversation.
The average overall satisfaction for the program was 4.2 out of 5 (4 corresponding to satisfied and 5 corresponding to extremely satisfied). 4/5 participants agreed that they would continue the program if they had the opportunity.
Closing Thoughts
An online wellness program via Google+ is a physically and financially feasible option for individuals with MS. Notable improvements in self-reported physical activity and exercise self-efficacy were observed in a short (4 week) time period. The program is not a perfect model: the technology is not ideal, and the program would be optimized for individuals with faster internet connections. The intervention is also more appropriate for individuals with moderate MS. Reimbursement remains another issue for therapists. Perhaps an individual could privately pay for a few sessions as the therapist organizes several individuals together and initiates the program. The therapist could direct the program to become self-autonomous as the individuals organize themselves for group exercise and self-help. This model frees therapists to initiate other groups and provide intermittent feedback to multiple groups. The online model could also be easily extended to other disciplines. Virtually any healthcare professional with an internet connection could be incorporated to provide instruction.
I welcome your thoughts and feedback regarding this program. If you would like to use any of the materials from the program, please feel free to do so. My hope is that these materials will help improve the care for individuals with MS and the broader population of individuals with neurological conditions.
Acknowledgements:
I owe a debt of gratitude to a number of individuals who made this entire experience possible. This program would not have been possible if I was not blessed to be a part of the MS STEP UP Program. Special thanks to Prudence Plummer for helping lay the foundation for this program and streamlining my ambitious dreams. I want to thank my committee members Kaye Gooch and Diane Meyer who provided feedback and helped with recruitment. Thanks to Angela Rosenberg for crafting MS STEP, sparking my interest in working with individuals with MS, and playing a key part in my UNC admission. Thanks to previous MS STEP UP Scholars for your mentorship. And thanks to my church family, who have been a constant source of encouragement and life for the last three years.
References:
- Asano M, Duquette P, Andersen R, Lapierre Y, Mayo NE. Exercise barriers and preferences among women and men with multiple sclerosis. Disabil Rehabil. 2013 Mar;35(5):353-61.
- Kasser SL, Kosma M. Health beliefs and physical activity behavior in adults with multiple sclerosis. Disabil Health J. 2012 Oct;5(4):261-8.
- Dlugonski D, Joyce RJ, Motl RW. Meanings, motivations, and strategies for engaging in physical activity among women with multiple sclerosis. Disabil Rehabil. 2012;34(25):2148-57.
- Motl RW, McAuley E, Snook EM. Physical activity and multiple sclerosis: a meta-analysis. Mult Scler. 2005 Aug;11(4):459-63.
- Dean E. Physical therapy in the 21st century (Part I): Toward practice informed by epidemiology and the crisis of lifestyle conditions. Physiotherapy Theory and Practice. 2009; 25(5-6): 330-353.
- Motl RW, Dlugonski D, Wójcicki TR, McAuley E, Mohr DC. Internet intervention for increasing physical activity in persons with multiple sclerosis. Mult Scler. 2011 Jan;17(1):116-28.
- Carter AM, Daley AJ, Kesterton SW, Woodroofe NM, Saxton JM, Sharrack B. Pragmatic exercise intervention in people with mild to moderate multiple sclerosis: a randomised controlled feasibility study. Contemp Clin Trials. 2013 Jul;35(2):40-7.
- Learmonth YC, Marshall-McKenna R, Paul L, Mattison P, Miller L. A qualitative exploration of the impact of a 12-week group exercise class for those moderately affected with multiple sclerosis. Disabil Rehabil. 2013 Jan;35(1):81-8.
3 Responses to “Testing the Feasibility of an Online Wellness Program for Individuals with MS”
Joseph Miller
Mark,
Thank you for your complements. Throughout my entire presentation, I kept asking myself “is this feasible and reproducible.” With all of my commitments this semester, I still managed to make this happen, so I think the overall conclusion is yes, especially with the improving technology. As for your question, I think the platform could operate as both as a self-help group and/or a wellness program. I think it’s important to consider your audience whenever you’re setting up any program. Self-help groups work for individuals across varying severities; those who have had a condition for a while can really give some great advice for those newly diagnosed. However, this same benefit does not carryover to exercise. When you exercise, you want to be with someone who’s either at your level of conditioning or someone who’s just at the next level (not someone who’s 10 levels above or below you). In addition, I do not think this type of wellness program is appropriate for all individuals. Those with more mild presentations would probably benefit from going to fitness centers or aerobic training (like walks). Similarly, those who have more severe cases probably need individuals care (though chair yoga may be an option for this population). The one participant who had mild MS admitted to me that she thought that the “exercises were boring,” but I think it’s important to highlight that the program still improved her exercise self-efficacy. This participant got back involved with her gym and was doing multiple sessions per week with her personal trainer. So, while the program may not be a long-term solution for everyone, I think it has potential to benefit every patient in some capacity.
Prue: I appreciate your complements as well. It means a lot coming from you. And I completely agree that we should encourage exercise in the community. Getting out and about also improves vitamin D, which is associated with better outcomes for individuals with MS.
Joe
Prue Plummer
Joe,
It is wonderful to see your vision come to life! It seems from the feedback in this initial group that the online modality may be most suitable for individuals with more severe impairments. We probably still should encourage those with more mild MS to continue to get out into the community as much as possible, including to attend exercise sessions.
I know there was a lot of preparation and behind the scenes work to put this together and execute it. You are to be commended for the dedication and effort.
I have enjoyed getting to know and working with you as part of the MS STEP UP program. You’ve shown tremendous dedication to your own learning, and that trait will serve you well in your career.
Congratulations on the successful completion of this great project!
Prue
Mark Boles
Joe,
Very cool capstone project! I can tell you put a lot of effort into making this project and I believe it paid off. I have a lot of respect for the MS scholars like yourself who dedicate significant amounts of time into helping this population of people, and your capstone really shows that dedication. You obviously ran into a couple bumps in the road with the technology and slow internet connection, but I truly think you are on to something that has a lot of potential. Even with the minor technical issues that you ran into your program still seemed to be successful for the majority of your participants. I am familiar with various support groups that are held at physical locations for individuals who have had an amputation, stroke, TBI, etc.; do you think that a similar virtual setup that you have described in your capstone could be a real possibility in the future for these populations as technology improves? Or do you think this kind of virtual setup would be better used as an addition to a support group rather than a substitution? It seems that technology is becoming a bigger and bigger part of healthcare each year so I’m just curious to hear your viewpoint. Thanks for sharing the resources from your project. This is something that I definitely want to check more into. Excellent job!
Mark