Created by: Korre Scott
For my capstone, I used and analyzed data from my fall research elective. I wanted to use my elective credits and this capstone project as a way to explore the research process, specifically for a population I’m interested in working with. I worked alongside Mike Lewek to determine how to make walking more energetically efficient for individuals with chronic stroke. This was a single session intervention that involved healthy control subjects and subjects post-stroke walking on a treadmill for five randomly ordered conditions. My portion of the project focused on implementing a cognitive-motor dual-task intervention to a walking condition designed to increase paretic limb propulsion throughout the swing phase of gait. I expanded my knowledge of this topic by reviewing the evidence for dual-task interventions on decreasing spatiotemporal asymmetries for individuals with chronic stroke during our Evidence-Based Practice II course. Based off of our research, I submitted an abstract to the UNC Human Movement Science and Biomechanics Research Symposium and presented a poster at the event in February, 2016. I then created a manuscript of the findings, which is posted below. My advisor, Mike Lewek, and research partner, Kelly Hewitt, have been invaluable resources throughout this entire process, and Dr. Prue Plummer has provided guidance throughout the writing process.
THE INFLUENCE OF COGNITIVE-MOTOR INTERFERENCE ON ATTENTIONAL RESOURCES DURING A TREADMILL WALKING INTERVENTION DESIGNED TO ASSIST WITH PARETIC PROPULSION
1Korre Scott, 1Kelly Hewitt, 1Prudence Plummer 1,2Michael Lewek
1Division of Physical Therapy, University of North Carolina at Chapel Hill
2Human Movement Science Curriculum, University of North Carolina at Chapel Hill
Introduction: Patients are often left with gait difficulties following a stroke. While walking recovery remains an import goal for rehabilitation, individuals continue to have an energetically inefficient gait. Rehab interventions should target propulsion for smooth forward progression during walking. However, more cognition may be required during the relearning process and interventions may not be as effective if patients cannot focus their attention to the motor task. The purpose of this study is to determine the effect on energy cost of walking and paretic peak hip extension of adding a cognitive-motor dual-task intervention to a treadmill intervention that assists with propulsive forces.
Methods: Six participants with chronic stroke (>6 months post-stroke) and 8 unimpaired control subjects participated in this single session study. We recorded gas exchange (VO2 inspired/VCO2 expired) on a breath-by-breath basis using a portable metabolic cart (Cosmed) while subjects walked on a dual-belt instrumented treadmill. Subjects completed three randomly ordered walking conditions for up to 5 minutes, with 5 minutes rest between conditions: 1) propulsion assistance (Anterior); 2) propulsion assistance with concurrent cognitive task (Dual-task); and 3) control. Propulsion assistance was provided to reduce anterior center of mass velocity fluctuations using theraband. Reaction time data was collected from each participant as they completed a 2-back task during treadmill ambulation. The average VO2 over the final minute of each condition was compared separately for each group between conditions using a repeated-measures ANOVA, with paired samples t-tests used for post-hoc analysis, as necessary.
Results: No statistically significant changes in cost of transport (COT) were observed between the Anterior and Dual conditions in either group (p=0.140). Similarly, no difference in peak hip extension was observed between the Anterior and Dual conditions (p=0.727). Accuracy of the cognitive task was not altered during the dual-task condition compared to the single-task condition (Control: p=0.717; Stroke: 0.659).
Discussion: The results do not support the original hypothesis, as the addition of a cognitive component to a treadmill intervention did not increase energy expenditure. Individuals appear to focus on the cognitive task and do not sacrifice task accuracy in order to attend to the walking intervention. Propulsion assistance provided by the theraband while walking on the treadmill may not have required as many attentional resources as other gait training or over ground walking scenarios. Thus, it is possible that treadmill walking interventions that assist with smooth forward propulsion are feasible interventions because they reduce the energy cost of walking while not requiring individuals to focus their attentional resources on the walking task. Further study is required to determine the potential positive or negative effect of a concurrent cognitive task on motor training post-stroke.
Introduction
Stroke is a leading cause of long-term disability in the US [1], with many individuals limited in their mobility by persistently slow, asymmetric, and energetically inefficient gait [2,3]. Gait restoration has been recognized as a main goal during rehabilitation, as only a small proportion of individuals can walk well enough to function fully in the community after a stroke [4]. Motor impairments from stroke increase the attentional demands of motor performance, further limiting community ambulation and walking ability [5]. There is competition for attentional resources when motor and cognitive tasks are performed simultaneously. Interventions that focus on specific motor impairments that limit walking following stroke may not be as effective if individuals cannot adequately attend to the desired motor task.
There are several motor deficits that potentially contribute to gait dysfunction following stroke. Individuals with impaired paretic limb propulsion often walk with a longer paretic step length and likely compensate by generating greater propulsive impulses in the non-paretic limb [6] Although the increased non-paretic propulsion may be a successful compensation with respect to walking speed,[7] it may have a detrimental effect on energy cost. The energy cost of gait is higher for individuals post-stroke due, in part, to an increase in mechanical work by the non-paretic limb to lift the body’s center of mass (COM) [3]. Providing propulsion assistance for the paretic limb may help that limb accelerate the body’s COM forward, and reduce the non-paretic limbs compensation. This may improve energy cost, which is known to be high when the legs do not provide symmetric push off [8].
Cognitive-motor interference has become an area of focus following stroke, and occurs when simultaneous performance of a cognitive and a motor task cause decreased performance in one or both tasks [10,11]. Throughout the day, individuals are faced with tasks that require the simultaneous execution of two or more cognitive and motor activities. By itself, walking is a relatively automatic process and does not involve cognitive control until old age [12]. Motor impairments that result from stroke increase the attentional demands of gait, leaving gait to be less automatic than before the stroke [11]. In return, increased attentional demands required for gait limit the available attentional resources to attend to other things while walking, such as a simultaneous cognitive task. The type of interference resulting from cognitive-motor dual tasking decreases gait speed and stride length in individuals with chronic stroke, potentially due to prioritization of attending to the cognitive task at the cost of gait performance [11,13,14]. Gait training may further increase the attentional demands of walking, as the patient must focus on verbal cues and instructions from the therapist while paying attention to their motor performance. Therefore, if dual-task capacity is limited, motor learning may be hampered. Implementing a novel gait training intervention may increase attentional requirements and have an impact on learning the desired motor task.
It has previously been determined that gait alterations on a treadmill are transferable to over-ground walking [15]. Individuals with chronic stroke are capable of improving step length, gait speed, and cadence with the addition of a cognitive-motor task during treadmill specific gait training [16,17]. However, much of this research involves participants walking at a self-selected comfortable speed with no external alterations to their gait. One potential alteration is to provide propulsion assistance to the paretic limb, as increased propulsive impulse is positively related to leg extension and negatively related to the hip flexor impulse [18]. To date, no study has examined the effects on gait of adding a cognitive task to a gait-training paradigm that assists with propulsive forces.
The purpose of this study was to determine the effect of adding a cognitive task to a novel gait-training intervention on a) energy cost of walking and b) joint kinematics. We hypothesized that implementing a cognitive task during treadmill walking with novel propulsion assistance will increase the cost of walking compared to walking with propulsion assistance without a simultaneous cognitive task. This hypothesis is based on the expected added energetic cost associated with the cognitive task [9], and the potential decline in use of the propulsion assistance with diminished attentional resources available for the motor task. In addition, we hypothesized that paretic peak hip extension will decrease when a cognitive task is implemented with a propulsion assistance.
Methods
Participants
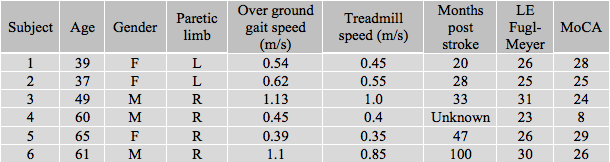
We recruited six participants with chronic (>6 months) stroke (females, n=4; age, 51.83 ± 11.97 y; left limb tested, n=4; mean treadmill speed, 0.6 ± 0.26 m/s) and eight unimpaired control subjects (females, n=5; mean age, 25.75 ± 3.01 y; left limb tested, n=2; mean treadmill speed, 1.3 ± 0.14 m/s). All subjects were able to walk over ground without physical assistance. Participants were excluded if they displayed 1) neurologic (except for a stroke in the Stroke group), cardiovascular, or orthopedic conditions that might have affected their ability to ambulate at a comfortable gait speed on treadmill, 2) balance deficits or unexplained falls not related to the stroke, or 3) cognitive or communication impairments that could hinder understanding of the purpose or procedures of the study. All participants read and signed a consent form approved by the Institutional Review Board at the University of North Carolina at Chapel Hill.
Data Collection
All participants completed a single session of walking, during which kinematic, kinetic, and metabolic cost of walking measures were collected. Individuals completed three randomly-ordered walking conditions for up to 5 minutes on a dual-belt instrumented treadmill (Bertec Corp, Columbus, OH), with at least 5 minutes of rest between conditions. Conditions included: 1) propulsion assistance, 2) propulsion assistance with concurrent cognitive task (dual-task), and 3) control walking. Treadmill speed was targeted between 80-100% of over ground comfortable walking speed, which was determined by each participant performing two passes over a Zeno Walkway (ProtoKinetics, Havertown, PA). Propulsion assistance was provided to assist with anterior COM movement, with a target peak pulling force set at 10% body weight [19]. The propulsion assistance was designed to assist with forward progression of the COM only during unilateral propulsion phase of gait. The device providing assistance provided by an elastic element attached to the front of the participant’s waist, looped over the front of the treadmill, and attached at the ankle of the impaired (or tested) limb. Prior to beginning the first randomly-ordered walking condition all subjects completed a 5-minute practice trial of a “two-back task” in which they were seated. During the two-back task, subjects listened through a headset to a list of letters which were separated by 3 seconds. Subjects were provided with a button to push as quickly as possible when they heard a letter repeated that was read 2 letters previously. The button push eliminated any difficulty with the use of the Cosmed mask for measuring O2 consumption. The two-back task was performed during the dual-task condition, with the input button fixed to a side handrail of the treadmill for participants needing additional support. All participants wore an overhead harness for safety while walking, which did not provide unweighting or restrict lower extremity movements.
Lower extremity and pelvic movement data were recorded using an 8-camera motion capture system (Vicon, Denver, CO) sampleing at 120 Hz while participants walked on the treadmill. Limb segments were tracked with retroreflective markers attached to the subject’s pelvis, legs, and feet. Concurrently, we sampled ground reaction force (GRF) data from the treadmill and the anterior pulling force from a tension-compression load cell (MLP-150; Transducer Techniques) at 1200 Hz. Gas exchange (VO2 inspired/VCO2 expired) data were recorded on a breath-by-breath basis using a portable metabolic cart (K4b2; Cosmed). Average reaction times and accuracy of the two-back task during the dual-task condition were measured using DirectRT software (Empirisoft, New York, NY).
Data Management
Metabolic data (VO2) were averaged over the last minute for each condition and converted to Cost of Transport by dividing VO2 by the subjects mass and walking speed. Kinematic and kinetic data were calculated using Visual 3D software (C-motion, Germantown, MD) based on anthropometric measurements. In particular, we focused on the peak hip extension angle, given its known importance to propulsive forces [20]. A custom design LabVIEW program (National Instruments Corp, Austin, TX) was used to determine the peak hip extension angle and the peak anterior pulling force to the COM that was supplied by the elastic band.
Data analysis
All data were analyzed using SPSS (version 23; Chicago, IL). We performed 4 separate two-way repeated measures ANOVAs (repeated for condition) to compare the COT, 2-back task accuracy, peak anterior pulling force, and the peak hip extension angle between groups. Paired samples t-tests and one way repeated measures ANOVAs were used as post-hoc tests, when appropriate. We used an α=0.05 to indicate significance.
Results
The demographic data for participants is described in Tables 1 and 2. Participants in the Control Group had a mean comfortable walking speed of 1.34 ± 0.17 m/s. Participants in the Stroke Group had a mean comfortable walking speed of 0.705 ± 0.327 m/s.
Table 1. Control Group: Individual Demographics
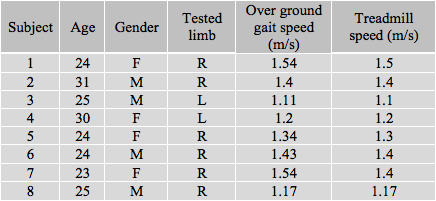
Table 2. Stroke Group: Individual Demographics
We observed a significant difference in the magnitude of pulling force between the different conditions (P=<0.001; η2p=0.954). Specifically there was more force applied during the Anterior (p<0.001) and Dual (p<0.001) conditions compared to the Control condition. Notably, there was no difference in applied pulling force between the Anterior and Dual conditions (P=0.879). We also observed no difference in the magnitude of pulling force between the Stroke and Control groups (P=0.242; η2p=0.122), and observed no significant interaction effect (P=0.390; η2p=0.082).
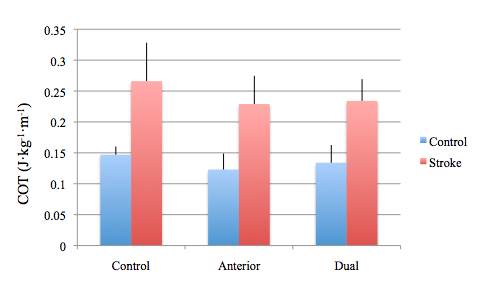
Mean values for cost of transport (COT) can be observed in Figure 1. Overall, the Stroke group exhibited significantly higher COT than the Control group (p<0.001; η2p=0.743). We also observed a significant main effect for condition for COT (P=<0.001; η2p=0.515). There was significantly lower COT during the Anterior (p<0.001) and Dual (p=0.013) conditions compared to the Control condition. However, we observed no difference in COT between the Anterior and Dual conditions (p=0.140). Both groups responded similarly between conditions, as exhibited by no significant interaction effect (P=0.316; η2p=0.092).
Figure 1. Cost of Transport for each treadmill-walking condition
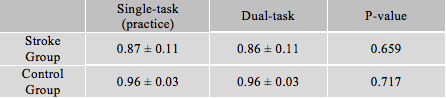
Accuracy values during the two-back task for each group during the single- and dual-task conditions can be seen in Table 3. We observed a lack of a dual-task effect (P=0.872; η2p=0.002) on the cognitive task (2-back task) based on the comparable level of accuracy during single and dual task conditions for both groups (P=0.548; η2p=0.031). However, the Control group had significantly greater accuracy than the Stroke group (P=0.028; η2p=0.344) during the 2-back task.
Table 3. Accuracy of Two-Back task
Data for peak hip extension revealed significant main effect for condition (P=<0.001; η2p=0.511), with less hip extension noted during the Anterior (p=0.002) and Dual (p=0.006) conditions compared to the Control condition. No difference in peak hip extension was observed between the Anterior and Dual conditions (p=0.727). Likewise, we observed no difference between groups (P=0.495; η2p=0.043) and no interaction effect (P=0.947; η2p=0.005).
Discussion
The hypothesis that the addition of a cognitive task during treadmill walking with propulsion assistance will increase the energy cost of walking compared to walking with propulsion assistance alone was not supported by these data. In both groups, adding propulsion assistance reduced metabolic COT in both the Anterior and Dual conditions compared to the Control condition, with no difference between Anterior and Dual conditions.
The addition of the cognitive component (i.e., two-back task) was chosen to divert attentional resources from the desired novel motor task at hand. Despite consistent accuracy from the single- to dual-task trials in both groups, the two-back task was difficult for the Stroke group, who averaged 86% during the dual-task condition. This indicates that use of the 2-back task requires increased attentional resources with normal aging and should have allowed for interference in the walking task due to competition for attentional resources between the cognitive and motor task [12]. If the novel walking task with propulsion assistance really required greater attentional resources to make use of the assistance, than we would have expected to see a decrease in cognitive performance. That cognitive performance did not decrease during the Dual task condition, suggests that the novel walking task was not using significant attentional resources. Subjects were still able to reap the metabolic benefits from the imposed intervention, even while sharing attentional resources with the challenging 2-back task. Utilizing the two-back task during the study was thought to be sufficient for inducing a deficit in motor performance, but the results for COT and peak hip extension suggest otherwise.
Another consideration involves the difficulty level of the motor task. It is possible that walking on the treadmill with a theraband providing propulsion assistance does not increase attentional demands to the same degree as other simultaneous motor tasks. Individuals demonstrate reductions in task accuracy, walking speed, and walking accuracy when attempting to complete a difficult ambulation task while simultaneously performing a memory recall task [21]. In this study, walking with propulsion assistance from the theraband may not have caused a deficit in the cognitive task because the motor task may not have been as attentionally demanding as other motor tasks. In addition, motor performance was enforced as participants walked on a treadmill at their selected walking speed, which may have prevented deficits in motor performance (i.e., COT) during the Dual condition.
Importantly, participants in both groups displayed less peak hip extension with the addition of an anterior-directed pull. Other forms of treadmill walking have been able to elicit increased paretic hip extension through increased treadmill speeds [20]. In this study, we believe that the reductions in hip extension are the result of participants not allowing their tested limb to extend to its full capacity due to the resistance band simultaneously pulling the limb forward.
Limitations of this study include a small sample size for both groups. The target pulling force was set at 10% body weight based on previous research with healthy controls, however, this may not have been the proper target to use within a population of individuals with chronic stroke [19]. Also, all participants were instructed in the two-back task prior to the single- and dual-task conditions, but were not instructed to push the input button as quickly as possible, which may have had an impact on task accuracy results.
Conclusion
The results do not support the original hypothesis, as the addition of a cognitive component to a treadmill intervention that assists with paretic propulsion on decreasing COT is similar to propulsion assistance alone. Individuals appear to focus on the cognitive task and do not sacrifice task accuracy in order to attend to the walking intervention. Propulsion assistance provided by the theraband while walking on the treadmill may not have required as much attentional resources as other gait training or over ground walking scenarios. Thus, it is possible that treadmill walking interventions that assist with smooth forward propulsion are feasible interventions because they reduce the energy cost of walking while not requiring individuals to focus their attentional resources on the walking task.
References:
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics-2016 update: A report from the american heart association. Circulation. 2016;133(4):e38-e360.
- Lewek MD, Randall EP. Reliability of spatiotemporal asymmetry during overground walking for individuals following chronic stroke. J Neurol Phys Ther. 2011;35(3):116-121.
- Stoquart G, Detrembleur C, Lejeune TM. The reasons why stroke patients expend so much energy to walk slowly. Gait Posture. 2012;36(3):409-413.
- Lord SE, McPherson K, McNaughton HK, Rochester L, Weath- erall M. Community ambulation after stroke: how important and obtainable is it and what measures appear predictive? Arch Phys Med Rehabil 2004;85:234-9.
- Plummer P, Eskes G, Wallace S, et al. Cognitive-motor interference during functional mobility after stroke: State of the science and implications for future research. Arch Phys Med Rehabil. 2013;94(12):2565-2574.e6.
- Balasubramanian CK, Bowden MG, Neptune RR, Kautz SA. Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch Phys Med Rehabil. 2007;88(1):43-49.
- Bowden MG, Balasubramanian CK, Neptune RR, Kautz SA. Anterior-posterior ground reaction forces as a measure of paretic leg contribution in hemiparetic walking. Stroke. 2006;37(3):872-876.
- Farris DJ, Hampton A, Lewek MD, Sawicki GS. Revisiting the mechanics and energetics of walking in individuals with chronic hemiparesis following stroke: From individual limbs to lower limb joints. J Neuroeng Rehabil. 2015;12:24-015-0012-x.
- Kodesh E, Kizony R. Measuring cardiopulmonary parameters during dual-task while walking. J Basic Clin Physiol Pharmacol. 2014;25(2):155-160.
- Plummer P, Villalobos RM, Vayda MS, Moser M, Johnson E. Feasibility of dual-task gait training for community-dwelling adults after stroke: A case series. Stroke Res Treat. 2014;2014:538602.
- Plummer P, Eskes G, Wallace S, et al. Cognitive-motor interference during functional mobility after stroke: State of the science and implications for future research. Arch Phys Med Rehabil. 2013;94(12):2565-2574.e6.
- Lovden M, Schaefer S, Pohlmeyer AE, Lindenberger U. Walking variability and working-memory load in aging: A dual-process account relating cognitive control to motor control performance. J Gerontol B Psychol Sci Soc Sci. 2008;63(3):P121-8.Yang YR, Chen YC, Lee CS, Cheng SJ, Wang RY. Dual-task-related gait changes in individuals with stroke. Gait Posture. 2007;25(2):185-190.
- Hyndman D, Ashburn A, Yardley L, Stack E. Interference between balance, gait and cognitive task performance among people with stroke living in the community. Disabil Rehabil. 2006;28(13-14):849-856.
- Savin DN, Morton SM, Whitall J. Generalization of improved step length symmetry from treadmill to overground walking in persons with stroke and hemiparesis. Clin Neurophysiol. 2014;125(5):1012-1020.
- Yang YR, Wang RY, Chen YC, Kao MJ. Dual-task exercise improves walking ability in chronic stroke: A randomized controlled trial. Arch Phys Med Rehabil. 2007;88(10):1236-1240.
- Kwon OH, Woo Y, Lee JS, Kim KH. Effects of task-oriented treadmill-walking training on walking ability of stoke patients. Top Stroke Rehabil. 2015.
- Peterson CL, Cheng J, Kautz SA, Neptune RR. Leg extension is an important predictor of paretic leg propulsion in hemiparetic walking. Gait Posture. 2010;32(4):451-456.
- Gottschall JS, Kram R. Energy cost and muscular activity required for propulsion during walking. J Appl Physiol (1985). 2003;94(5):1766-1772.
- Tyrell CM, Roos MA, Rudolph KS, Reisman DS. Influence of systematic increases in treadmill walking speed on gait kinematics after stroke. Phys Ther. 2011;91(3):392-403.
- Hsiao H, Knarr BA, Higginson JS, Binder-Macleod SA. Mechanisms to increase propulsive force for individuals poststroke. J Neuroeng Rehabil. 2015;12:40-015-0030-8.
- Lindenberger U, Marsiske M, Baltes PB. Memorizing while walking: Increase in dual-task costs from young adulthood to old age. Psychol Aging. 2000;15(3):417-436.
One Response to “The influence of cognitive-motor interference on attentional resources during a treadmill walking intervention designed to assist with paretic propulsion”
Michael Lewek
Korre,
You did a wonderful job on this entire research project. This capstone is the culmination (so far) of all the hard work that you have done since the fall semester. Over the course of the past year you have spent countless hours learning to independently use just about every piece of equipment in the lab, test 20+ subjects, analyze and interpret the data, and present them in a clear and compelling manner. You should be proud of your efforts and your outcome. We will work to get this out for publication in the next few months and this will make an important contribution to the literature.
Well done.
BTW, I’m posting the same thing to Kelly, since you two worked as such a great team together for the past year.
Mike