
Bridging the Gap: Transition from Hospital to Home for SCI
Sara Galante, SPT & Austin White, SPT
Background
Our passion for patient education and working with individuals who have neurological injuries brought us together as teammates for our second year “Managing Contemporary Practice” course project. Although our idea for the project did not fit that class’ learning objectives, we were passionate about pursuing the idea later. During our second year rotations, we gained the background needed in order to pursue filling a need in the current system. We knew this was a big idea that would take a lot of work, and luckily, the Capstone curriculum was the perfect opportunity to create the first draft of our passion project that we hope to expand throughout our future careers. We worked together as a team on every aspect of this project, we shared the same adviser and committee, and now we share a Capstone website for you to see the culmination of our hard work.
Sara’s Background
My passion for rehab began volunteering on UNC’s 7th floor inpatient unit, organizing the assistive devices closet and helping with wheelchair follows. I further got to explore that passion on my second rotation at inpatient rehab in Charlotte, working on the Spinal Cord Injury (SCI) team and conducting patient education classes on topics related to transition to home. I knew that logistically this was the perfect opportunity for education, yet some patients were worn out, confused by the language, or weren’t psychologically ready to hear this information. Now they were missing out on information they needed to know, information that could keep them out of the hospital later. This was anecdotally confirmed for me on my third rotation, when I saw one of my previous patients from rehab admitted to acute care with secondary complications from his injury. I called Austin on my way home this day and told her about how our idea had come full circle.
Austin’s Background
My heart has always been with inpatient rehab and patients with neurological injuries. I find it really fulfilling to work on functional mobility and provide education to patients and their caregivers to facilitate the transition back home after a (typically) traumatic experience. While witnessing a family friend navigate his return home after an SCI, I noticed the “telephone effect” that occurred as he and his primary caregiver (his wife) had to teach new hired caregivers how to perform dependent transfers based on what they remembered from the overwhelming time in inpatient rehab. Despite the wonderful care and education while in rehab, there was still a gap in terms of caregiver resources to help ease the burden on the family to train other caregivers. During my third rotation at an inpatient rehab facility in Wilmington, I too noticed the impact of learning readiness on patient education. Therefore, when Sara called on her way home from work one day, we decided Capstone was an opportunity to pursue our patient education idea.
Statement of Need
While our ultimate hopes and dreams are that this could one day turn into an all-inclusive website for all levels of SCI covering many different topics, we have narrowed our focus for this project. The functional level of the target audience will include those that have periscapular and shoulder mobility, lack hand function/fine motor control, and require assistance from caregivers for ADLs and transfers. This subgroup is important to address within the SCI population, as their limited independent mobility requires the development of direction of care skills to communicate with caregivers to optimize their autonomy.
Conversations with healthcare providers, caregivers, individuals with SCI, and our literature review revealed that more focus should be devoted to the transition period from hospital to home. Barriers arise after the transition to home, as evidenced by the development of secondary conditions, hospital readmissions, and health complications in the SCI population.1-4 This Capstone idea to create easily accessible, online videos will help bridge some of the education gaps during the caregiver shift from the PTs and nurses in rehab to the families and spouses at home.5
A current online resource for the SCI population called “Voices of Experience” does include some online educational videos; however, it does not include direction of care, which is why the need for our particular product still exists.
Overview & Purpose
Our Capstone project is intended to meet the above need through evidence-based strategies, including the intentional timing, use of peer mentors, online video format, and topic of direction of care.
The available literature indicates adult learners need to be ready for learning in order to successfully implement new information;6 however, with the coping that is initially required after SCI, many are unable to learn when they have access to education at the hospital before the transition to home.7-9
Education via peer mentoring is well supported in the literature,1,2,10 yet the outpatient healthcare providers all described how difficult it is to access peer mentors in the community as compared to while in the hospital. In contrast to other supportive relationships, the benefits of peer mentors include credibility and normalization as well as increased quality of life and self-efficacy.2,10
The online video format is an effective education delivery method, as evidenced by the nearly six-time greater reach of the online format in just one third of the amount of time with a wide geographic distribution of the audience.5 Furthermore, given the functional level of our target audience, online videos decrease the amount of assistance required from caregivers as compared to in-person education sessions.
Successful direction of care incorporates self-awareness of the body, clear and specific communication, confidence to self-advocate, problem-solving skills, patience, and flexibility.4 The current development of an outcome measure to directly assess the ability of individuals with SCI to direct care and caregiving suggests that this is a topic of growing interest and importance in the SCI population.4
Health Literacy
Many standard-of-care education formats (i.e. generic handouts provided during rehab) are delivered via methods that are not health-literacy friendly, and the recipients fail to understand and find relevance in the material.2 The use of peer educators helps achieve health literacy in our videos by limiting the amount of medical terminology used and lowering the reading level of material. In addition, a video format removes the reading comprehension component, making the material more accessible. From our literature review, we know there is a lack of research examining health-literacy conscious patient education for individuals with SCI. However, utilizing the peer mentors under the direction of a PT is not harmful and qualitative data suggests that patients preferred peers.2,3,7-9,11
Products
Our evidence table and literature review provides evidence-based support for the strategies used in the two Capstone products.
We created two peer mentor videos on the topic of direction of care. Two different peer mentors were featured to relate to different members of the target audience.
Giovanna is a young adult who has a C6 incomplete SCI (ASIA B) who discusses her transition from hospital to home including how her relationships changed and what she wishes she knew during that time.
Paul is an older adult who has a C4 incomplete SCI (ASIA C) who discusses his transition from hospital to home including his experience hiring paid caregivers and current challenges while directing care. Paul also models how he directs care while eating dinner and changing his contacts.
Our ultimate goal is that these videos will eventually be housed on a website for all levels of SCI covering many different topics for individuals with SCI and their caregivers.
Evaluation
Due to extenuating circumstances, we were not able to visit the North Carolina Spinal Cord Injury Association (NCSCIA) support groups as originally planned to present and evaluate our videos in person. Therefore, to assess our videos, we reached out to individuals with SCI in the community and clinicians who frequently work with this population to watch the videos online and submit feedback on a Qualtrics survey. This led to a small sample size of 11 responses, including four responses from individuals with SCI. Some statements were not applicable to all viewers, and thus 11 responses were not recorded for every statement.
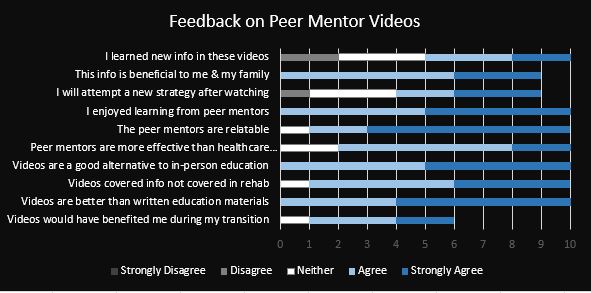
Consistent with the literature, all viewers enjoyed learning from a peer mentor with 54.55% strongly agreeing. The peer mentor was relatable for 90% of viewers including 20% who agreed and 70% who strongly agreed. All viewers agreed (36.36%) or strongly agreed (63.64%) that the video format was a better way to present this information than written formats currently used for most patient education. Again consistent with the literature, all of the viewers with SCI (n=4) agreed (50%) or strongly agreed (50%) that the peer mentor was more effective than other healthcare providers or experts at conveying this information.
Interesting comments included: “I would’ve enjoyed seeing it in rehab! Though, it might have scared me a little bit…” and “I think the patient should decide for themselves when to watch it and whether or not they want to.” These statements reflect our earlier instincts that the timing of this beneficial education will be different for everyone, meaning online access to the material fills this need. The evaluation step has led to feedback that indicates what videos are needed as we expand this project in the future.
Reflections
Sara’s Reflection
This has been one of the most challenging and rewarding experiences of PT school thus far. Growing up as a “creative type,” I always thought I would be pursuing an artistic avenue after college and while my path brought me to PT, I now realize I can do both. Learning a new skill (video and editing) for this project was daunting, but something I have been wanting to do for a while. The process of developing our final products challenged me to be creative yet realistic, something difficult as my ambition often exceeds my available hours in a day. An idea like this is necessary, and the world is changing so quickly that technology is one of the only avenues for communication and building relationships. Even though COVID-19 forced us to adapt and change direction on a few components of our project, I realize the potential of this idea now more than ever. Patients are still in the hospital, they would still benefit from learning from a peer, yet don’t have access to one.
This was also one of the first times that I searched for research and found almost nothing. The process of searching and writing the literature review over the past 2 semesters really made me grow my clinical reasoning skills and help solve a problem the literature hasn’t addressed yet. Maybe, in time, we will help answer these questions with research of our own. Another unintended benefit of the lack of literature was the professional connections we gained as we sought out expert opinions during this experience. I had a great excuse to converse with and pick the brains of some amazing mentors in this field from program developers, to other allied health professors, to previous CIs, and a PT I used to shadow as an undergraduate.
Finally, it is incredibly fulfilling for me to have the first step of a passion project with one of my best friends and amazing future colleagues. It’s been a hard three years of laughing, crying and every emotion in between and I don’t think I could have gone through this creative process with anyone but her. After several project pivots, new ideas, and brainstorming sessions, it’s amazing she still want to work with me on this but I am excited about being in it for the long-haul!
Austin’s Reflection
It has been an incredibly rewarding experience to discover a need and fill that gap with a tangible resource that can be used in the future. While I’m so proud of these two peer mentor videos for our Capstone project, I’m equally as excited about continuing this project with one of my dearest friends throughout our careers incorporating the feedback we received. It is really fulfilling to know this is the beginning of something that could be really special rather than just the end of an assignment.
Collaboration with several different key stakeholders has also been a highlight of the experience for me. I loved being able to connect and have conversations with interdisciplinary professionals (including PTs, OTs, and the chairman of the NCSCIA) from a wide range of settings and individuals with SCI at different stages of recovery in a variety of locations around the state (thank you social media!). These professionals have become valuable mentors and for that I am so grateful. This collaboration helped build my communication skills, but it also gave me so much perspective and respect for each and every voice as they all contributed valuable insight. The collaboration with key stakeholders also highlighted the fact that there is a clear need here, yet how to fill that need is difficult due to the individuality that accompanies learning readiness after a traumatic SCI and the emphasis on productivity for clinicians that limits time available for passion projects such as this one.
This experience has also been a learning lesson on the importance of flexibility, as this project took many pivots as we navigated stakeholder conversations and learned what was realistically possible. For example, while we originally planned to show an example of a dependent transfer, we also recognized the boundaries of respecting what our volunteers were comfortable with doing and sharing as it meant so much that they were willing to be so open about this vulnerable time in their lives. Another example was the impact of COVID-19, which limited our ability to incorporate committee and evaluation feedback into the final products. We could not re-film any interview segments based on feedback in an attempt to keep our peer mentors safe and healthy, but it further reiterated that this is the beginning (not the end) of this passion project.
Acknowledgements
First and foremost, we would like to give a huge thank you to Giovanna, Paul, and their families for opening up their homes and hearts to us. While in these videos they serve as peer mentors for individuals with SCI, their desire to help others by being open and vulnerable about a challenging time in their lives is something that we can all learn from.
To Dr. Vicki Mercer, PT, DPT, thank you for your patience with our pivots and for grounding us when narrowing the focus of our larger-than-life aspirations was necessary.
To Raheleh Tschoepe, MS, OTR/L, thank you for providing calm and tangible guidance during our creative struggles and introducing us to our peer mentors for these videos.
To Dr. Austin Leedy, PT, DPT, thank you for fostering love for this underserved patient population, bouncing ideas back and forth at coffee shops, and providing a unique perspective from the acute care setting when a patient’s journey begins.
To Dr. Audrey Osinski, PT, DPT, NCS, MSCS, thank you for connecting us with experts in the triangle, providing expertise yourself, and being involved from start to finish from initial brainstorming to problem-solving through the difficulties due to COVID-19.
To Debbie Meyers from the NCSCIA, thank you for your expertise that helped us narrow our focus early on and for inviting us to attend the local SCI support groups.
Finally, thank you to all of our classmates in the Class of 2020! Your support and love allowed us to grow and fearlessly pursue our passion despite the hard work it would take. Thank you for an amazing 3 years and we can’t wait to see the amazing group of clinicians you’ll be!
References
- Jones ML, Gassaway J, Sweatman WM. Peer mentoring reduces unplanned readmissions and improves self-efficacy following inpatient rehabilitation for individuals with spinal cord injury. J Spinal Cord Med.2019:1-9. doi:10.1080/10790268.2019.1645407.
- Chaffey L, Bigby C. Health Education by Peers with Spinal Cord Injury: a Scoping Review. J Dev Phys Disabil.2017;30(1):1-14. doi:10.1007/s10882-017-9569-6.
- Schubart J. An e-learning program to prevent pressure ulcers in adults with spinal cord injury: a pre- and post- pilot test among rehabilitation patients following discharge to home. Ostomy. Wound. Manage.2012;58(10):38-49.
- Zanca JM. Systematic Assessment of Caregiving Skill Performance by Individuals with Tetraplegia and Their Caregivers. Kessler Foundation.2017.
- Hoffman J, Salzman C, Garbaccio C, Burns SP, Crane D, Bombardier C. Use of on-demand video to provide patient education on spinal cord injury. J Spinal Cord Med.2011;34(4):404-409. doi:10.1179/2045772311Y.0000000015.
- Whiteneck GG, Gassaway J, Dijkers MP, et al. Inpatient and postdischarge rehabilitation services provided in the first year after spinal cord injury: findings from the SCIRehab Study. Arch. Phys. Med. Rehabil.2011;92(3):361-368. doi:10.1016/j.apmr.2010.07.241.
- Bernet M, Sommerhalder K, Mischke C, Hahn S, Wyss A. “theory does not get you from bed to wheelchair”: A qualitative study on patients’ views of an education program in spinal cord injury rehabilitation. Rehabil. Nurs.2019;44(5):247-253. doi:10.1097/rnj.0000000000000175.
- van Wyk K, Backwell A, Townson A. A narrative literature review to direct spinal cord injury patient education programming. Top. Spinal Cord Inj. Rehabil.2015;21(1):49-60. doi:10.1310/sci2101-49.
- May L, Day R, Warren S. Evaluation of patient education in spinal cord injury rehabilitation: knowledge, problem-solving and perceived importance. Disabil. Rehabil.2006;28(7):405-413. doi:10.1080/09638280500192439.
- Skeels SE, Pernigotti D, Houlihan BV, et al. SCI peer health coach influence on self-management with peers: a qualitative analysis. Spinal Cord.2017;55(11):1016-1022. doi:10.1038/sc.2017.104.
- Gassaway J, Jones ML, Sweatman WM, Young T. Peer-led, transformative learning approaches increase classroom engagement in care self-management classes during inpatient rehabilitation of individuals with spinal cord injury. J Spinal Cord Med.2019;42(3):338-346. doi:10.1080/10790268.2017.1385992.