Background:
Sports medicine and working in sports populations has appeals to me since before beginning the UNC DPT program. Prior to the DPT program, my background in exercise and sport science, coaching education, and interning as a strength and conditioning coach with UNC athletics for multiple years has fueled this passion. Throughout my DPT education I have worked on sport related topics where able. For example, topics explored thus far include plyometrics’ role in rehabilitation, subjective/objective load quantification methods for physical therapy, and patellar tendinopathy evidence-based rehabilitation guidelines, and predictive factors for return to sport (RTS) with bone-patellar-bone anterior cruciate ligament (ACL) grafts. I have also helped co-lead a sports journal club within my program and have been offered a position to complete a sports residency within the upcoming year.
When initially presented the project topic by Dr. Thoma and Dr. Franek, I immediately jumped at the opportunity. ACL rehabilitation is a big topic in sports physical therapy and one that is much more nuanced than other injuries. Strength measurements require more objective measures than manual muscle testing, a myriad of functional tests exist for quantifying knee function, and many other nuances (i.e. graft healing timelines, return to running, and return to jumping) require consideration. Understanding how to manage the RTS process and what criteria to utilize transfers over to other injuries as well for RTS. This project allowed me to inspect more closely the various criteria considered in ACLR including time, pain/effusion, range of motion, strength, functional performance, and outcome measures. I saw this Capstone project as an opportunity to become more familiar with the ACLR rehabilitation process rationale and how to specifically conduct testing in this population to better serve my patients in the future.
Statement of Need:
Anterior Cruciate Ligament reconstruction (ACLR) is performed approximately 175,000-250,000 times per year in the United States of America and cost greater than $2 billion.1,2 Approximately 65% of these injuries are treated via reconstruction surgery.3 Despite the volume research produced on ACLR and ACL injury in general each year, deficits still remain in the ability of physical therapists to adequately restore function and return individuals back to their sport. Current literature paints a grim picture of the outcome those undergoing ACLR may experience. Of those who receive ACLR surgery, up to 30% of these patients undergo another ACL rupture within a few years post reconstruction.1 Additionally, one meta-analysis found that only 72% of those receiving ACLR returned to their pre-injury level of activity at 2 years post-ACLR; 30-45% of patients do not RTS at all.4,5 Furthermore, other studies present various residual deficits, such as strength (eccentric and concentric) that persist for a minimum of 2 years after surgery.1,6 In fact, at 2 years post reconstruction, only 66% of individuals undergoing ACLR have ≥ 90% strength in the involved lower extremity compared to the uninvolved.1 Various authors suggest that injury rate is highest for young athletes returning to high level sport within the first 2 years after ACLR.7,8 Those athletes less than 20 years old who undergo ACLR have a 6-fold increase in odds of re-injuring the surgical knee and 3-fold increase in odds of rupturing the contralateral ACL.8 Those that return to sport within 1 year of ACLR are reported to be at a 15 times increased risk to suffer a second ACL tear than those lacking relevant medical history associated with their knee.7 Some authors such as the Multicenter Orthopaedic Outcome Network and Gundersen Health have developed rehabilitation guidelines to guide clinicians in assessing relevant criteria for RTS.9,10 Given the high prevalence of re-injury to the surgical knee or injury to the contralateral knee, lack of return to prior level of participation, and lack of patients passing return to sport (RTS) criteria, this evidence should be closely assessed to determine what criteria are most useful in guiding the clinician to adequately return these athletes back to sport.
Purpose:
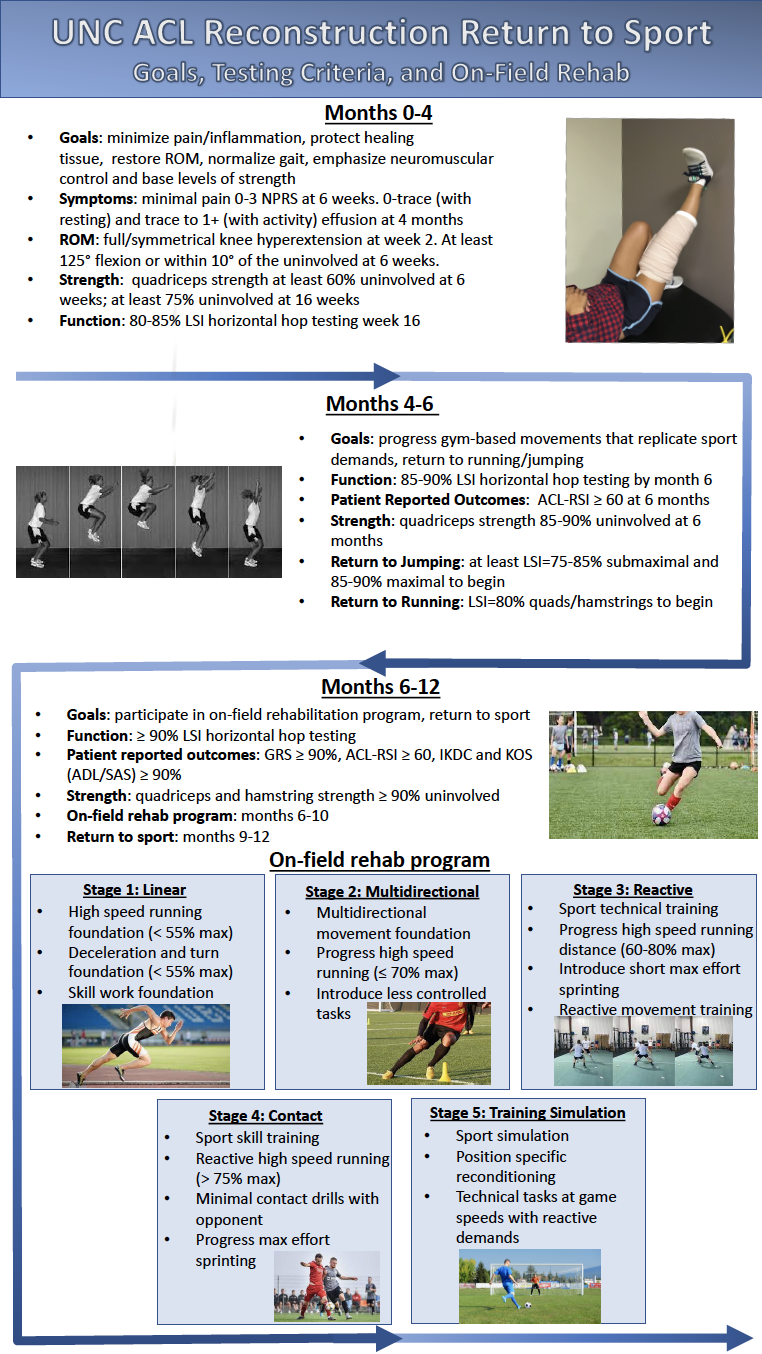
The aim of this project is to create an evidence-based guide for RTS testing criteria recommendations used in rehabilitation of ACLR that can be used by any clinician. This criterion hopes to provide a rationale for utilizing each criterion in assessing patients with ACLR, but also in providing instructions and practical recommendations for how to measure these criteria in the clinic. Another aim is to provide materials to facilitate tracking and assessment of RTS criteria between stakeholders within the RTS process (physicians, physical therapists, and patients). This includes utilizing infographics as means for providing an overview of the rehabilitation process to clinicians and education on the rehabilitation process to patients. Criteria include time, symptoms, range of motion, isolated strength, functional performance tests, on-field rehabilitation, patient reported outcomes, and physician clearance. For more in-depth information regarding the on-field rehabilitation portion, the clinician is referred to the Capstone project produced by my Capstone partner, Brandon Surber.
Products:
Products created include the following:
- RTS Criteria Narrative Review: Intended audience is for clinicians that will be using the RTS criteria for ACLR patients.
- RTS Criteria Instructions: Intended audience is for clinicians that will be performing tests in the clinic to ensure clinicians understand their options for testing and to standardize procedure for each test.
- RTS Scorecard Tracking Form: Intended audience is for clinicians. Directions for clinicians to appropriately perform assessments and repository of equipment/assessment options based on available equipment.
- RTS Infographic 1 (for clinician): Intended audience is for clinicians to use and describes the general overview of the entire rehab process and serves as a quick reference for the clinicians in determining where a patient is within the RTS process.
- RTS Infographic 2 (for athlete): Intended audience is for patients to view and provides a general overview of the entire rehab process and serves as a quick reference for the athlete in determining what they should be doing within the rehabilitation process at a given time point.
- RTS Presentation: Intended audience consists of clinicians such as Orthopedic Physicians, Physical Therapists, and Researchers interested in ACLR.
- RTS Presentation Video: Intended audience is for clinicians. Recorded lecture describing RTS criteria rationale, instructions, and resources created for clinicians.
- RTS Feedback Questionnaire: Intended audience is for clinicians to evaluate materials and provide feedback on aspects they liked and items that can be altered to improve the RTS criteria.
Evaluation:
Evaluation during this project was fairly continuous and consisted of frequent meetings, conversations, phone calls with members of the committee as well as my Capstone partner, Brandon. I met with Brandon frequently as needed to discuss various aspects related to the project and bounce ideas off one another. Brandon was a wonderful source for various literature I had not considered and incorporating those resources into the project. We also worked together on the infographics which allowed for editing and commenting asynchronously regarding progress of the materials. Zoom calls/phones calls were planned as needed with committee members to discuss various aspects of the project throughout the project’s duration and evaluate of any items needed refining. These began last fall with discussion of the project and future direction; these meetings were used as needed within the spring semester. Materials were provided to the committee for evaluation and feedback at midterm as well as prior to submitting materials for the Capstone website. Feedback from committee members was incorporated within the project at each point to ensure that the products were as comprehensive as possible. Another aspect of evaluation that is currently ongoing is the use of a Google Form to capture responses to evaluation of the materials that were sent to multiple stakeholders in ACLR rehabilitation at the UNC Meadowmont Clinic and physicians associated with UNC. I have only received one response at this time; however, I expect to receive more over the coming days. This information can be used to refine and further guide the direction of the RTS criteria as the committee members see fit for utilizing these materials in the future.
Self-Assessment:
During this project, I gained an enhanced understanding of the ACLR rehabilitation process as I had hoped. My clinical interests lie within sports, specifically jumping athletes, where this type of injury is prevalent. My knowledge regarding criteria to utilize to determine RTS and which criteria are most evidence-based has improved tremendously. Through the research process, I gained important skills is reading research, interpreting findings, and synthesizing finding from multiple studies and authors. I utilized many resources and became adept at following the research over multiple years to understand the complexities within each criteria such as Noyes and the first description of horizontal hop functional testing to Kotsifaki and how horizontal hopping may not be most indicative of knee function. I gained a newfound respect for the research process and also gained invaluable experience honing teamwork skills. I am very excited to have presented this material to stakeholders in ACLR within UNC, but also to present within a sport specific clinic at a later date. I believe the information I have learned is critical for becoming a responsible clinician within the sports setting. This information sheds light on just how prevalent re-injury is and what tools we have at our disposal to improve the RTS process; ultimately allowing for better treatment and outcomes for patients in the future. I feel much more comfortable knowing what test to utilize, how to interpret it, and when to use it within the ACLR process.
Acknowledgement:
I wanted to thank my project advisor, Dr. Louise Thoma, for all her help throughout this process. I would have been lost without your help and guidance whether meeting to discuss aspects of the project over Zoom or in answering questions over email. I appreciate all the edits and comments you provided to enhance my work and help refine the project into a final product that I was happy to help create. I wouldn’t have been able to complete this project without you helping lay the foundation for me to succeed. Thank you for allowing me the opportunity to work on such an interesting and intrinsically motivating project!
I also want to thank my other committee members, Dr. Madison Franek and Dr. Michael Lewek. You both were also instrumental in helping support me during this process and guiding me through the dense literature on the topic. The reference list related to the criteria that we began with were an amazing starting point that really helped narrow my search among the expansive literature on the ACLR. I appreciate all the Zoom calls, email communications, and phone calls to help make this project happen and to refine the material as needed.
Additionally, I would like to thank Brandon Surber, my partner within the Capstone project. We have been partners since the beginning of DPT school and discussing these complex topics in physical therapy is second nature. I appreciate all the time you sacrificed for Zoom calls to discuss the project, all the informal conversations about the profession, and for being a constant source to bounce ideas off of and to clarify the true meaning of research findings. I appreciate all the encouragement and feedback for my side of the project.
Last but not least, I would also like to thank the entire UNC DPT faculty and my classmates for all their help throughout the program and the relationships built. I appreciate you all greatly for pushing me to become a more proficient and knowledgeable clinician!
References:
- Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804-808. doi:10.1136/bjsports-2016-096031
- Spindler KP, Wright RW. Clinical practice. Anterior cruciate ligament tear. N Engl J Med. 2008;359(20):2135-2142. doi:10.1056/NEJMcp0804745
- Adams D, Logerstedt DS, Hunter-Giordano A, Axe MJ, Snyder-Mackler L. Current concepts for anterior cruciate ligament reconstruction: a criterion-based rehabilitation progression. J Orthop Sports Phys Ther. 2012;42(7):601-614. doi:10.2519/jospt.2012.3871
- Biau DJ, Tournoux C, Katsahian S, Schranz P, Nizard R. ACL reconstruction: a meta-analysis of functional scores. Clin Orthop Relat Res. 2007;458:180-187. doi:10.1097/BLO.0b013e31803dcd6b
- Buckthorpe M. Optimising the Late-Stage Rehabilitation and Return-to-Sport Training and Testing Process After ACL Reconstruction. Sports Med. 2019;49(7):1043-1058. doi:10.1007/s40279-019-01102-z
- Read PJ, Michael Auliffe S, Wilson MG, Graham-Smith P. Lower limb kinetic asymmetries in professional soccer players with and without anterior cruciate ligament reconstruction: nine months is not enough time to restore “functional” symmetry or return to performance. Am J Sports Med. 2020;48(6):1365-1373. doi:10.1177/0363546520912218
- Nagelli CV, Hewett TE. Should return to sport be delayed until 2 years after anterior cruciate ligament reconstruction? biological and functional considerations. Sports Med. 2017;47(2):221-232. doi:10.1007/s40279-016-0584-z
- Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42(3):641-647. doi:10.1177/0363546513517540
- Multicenter Orthopaedic Outcomes Network: ACL Rehabilitation Guidelines.
- Gundersen Health System: ACL Reconstruction Rehabilitation Program. November 2019.
4 Responses to “Anterior Cruciate Ligament Reconstruction Return To Sport Criteria- In Clinic Rehab”
Louise Thoma
Congratulations Ryan on a fantastic Capstone project and culmination of an incredible amount of work and synthesis of your personal interests and scholarly work! This project is a great example of working to implement research in practice. Evidence-based practice is always the goal, yet the realities of the clinic sometimes makes execution challenging. Tools and resources like these you have created make it easier for the clinician to implement in practice. I look forward to see how these tools are implemented at UNC and how you continue to develop these and other tools in your future practice!
Debbie Thorpe
Ryan
Really nice work! You created numerous valuable resources for clinicians and patients. It is evident that you delved deeply into the literature and did a nice job of synthesizing the evidence. I really like your info-graphics..easy to understand and complete. I would consider creating a voice thread for your presentation just in case you can not give it in person, as well, if faculty would like to get your permission to use it as content in the curriculum, the voicethread would be a good way to have the students view the presentation asynchronously.
Fantastic work!!
I think a Sports residency would be a great way to start your PT career!!
Good luck!
Debbie
swward
Hi Ryan,
This is an excellent capstone project. As a student who has spent more time outside of class learning about neurological and neuromuscular pathologies, I was really interested to dive into this sport specific musculoskeletal topic. I don’t want my focus on neuro PT to preclude me from learning more about sport, orthopedic, or general MSK rehabilitation and you (and Brandon) have given me a really good resource. I like that you provide really detailed instructions for the clinician while offering patient-centered information that is more easy to digest for the lay reader.
I don’t know exactly where I’ll end up working after graduation, but given the relatively high prevalence of ACL injuries, it is likely that I’ll work with patients at some stage along the rehab continuum. All of the products you created for clinicians offer an amazing level of detail that I, and others I’m sure, can appreciate. The Scorecard is a really nice idea that helps to take the guesswork out of rehabilitation progression and outcomes; I will definitely refer back to it and the other documents you created whenever I come across a patient with an ACL injury.
One suggestion I have for this page in general is for you to change the hyperlinks to open in a new tab instead of taking the reader away from this page and then needing to go back to return here. At least from my perspective, that sort of functionality really helps to ensure that someone can easily stay through to read all you have to offer, but is still able to follow along and look at links and attachments in tandem with your text.
Great job!
Sam Ward
Ryan Brooks
Sam,
Thanks so much for your kind words! I’m glad that you feel as though this is a good resource for clinicians as ACL rehabiliation has an immense amount of associate literature. My hope is this resource helps narrow down some of the important concepts and criteria in the rehabilitation/RTS process. The Scorecard’s goal is just to try and streamline communication between providers and may requires some discussion before so that orthopedic physicians are on board with the idea, but I feel it is a wonderful way to ensure the physician is up to date on how the patient is performing with therapy. Additionally, I appreciate you pointing the issue with the link to me. I am a little unfamiliar with building a website the way we had to for this Capstone so I didn’t even catch on to that specific issue with functionality. It is fixed now and hopefully makes navigating the page a little easier. Thanks again for your comment and suggestion Sam!