Author: Ashley Hodge, SPT
Advisor: Louise Thoma, PT, DPT, PhD
Committee Members: Sarah McAuliffe, PT, DPT & Carla Hill, PT, DPT, OCS, Cert MDT, CEEAA
Background
I was first made aware of the importance of attaining quadriceps strength and symmetry following knee injury and/or knee surgical procedure, while I was completing my physical therapy observation hours at an outpatient PT sports medicine clinic. From there, the importance of increasing quadriceps strength and achieving symmetrical bilateral strength was further reiterated throughout my PT school matriculation, as well as during my clinical rotations. I have always considered myself to be an inquisitive person that enjoys learning and have always desired to know and understand the “why” of subject matters. During our physical therapy academic careers we are taught that the quadriceps musculature may experience atrophy which may result in subsequent strength and functional deficits following injury to the joint and/or following a surgical procedure. Additionally, we are taught that persistent asymmetrical quadriceps strength can lead to higher rates of re-injury, increased rehabilitation time, and even subsequent disability. However, we are seldomly taught why the quadriceps musculature experiences these changes and which skilled PT interventions can specifically target these deficits in order to achieve long-term success. Therefore, I decided to participate in Dr. Louise Thoma’s post- traumatic osteoarthritis preceptorship, to learn more about the effects an injury to the knee can have on the joint as well as on the surrounding musculature. This preceptorship is where I first began to learn about and further research the topic of Arthrogenic Muscle Inhibition (AMI).
Statement of Need
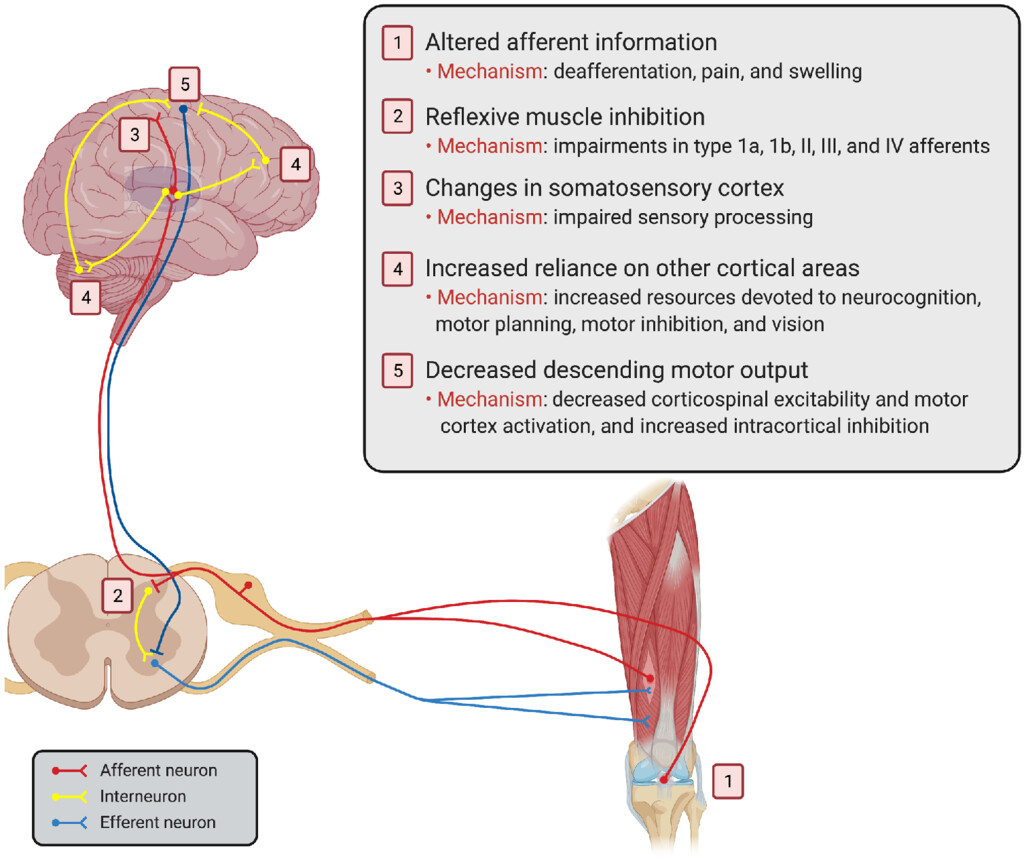
The importance of improving quadriceps strength of the involved limb and achieving symmetrical bilateral quadriceps strength following knee injury/surgical procedure is undoubtedly taught and emphasized throughout PT school and in clinical practice. Range of motion and pain relieving interventions, as well as therapeutic exercises are the typical interventions that are taught to help restore quadriceps strength in this population. However, despite participation in traditional rehabilitation, muscle weakness may persist. Which may result in persistent functional deficits and failure to meet therapeutic goals. Arthrogenic Muscle Inhibition is the proposed condition that may be resulting in this persistent muscle weakness despite full participation in physical therapy. However, AMI is rarely taught in PT school and practicing clinicians are often unaware of the condition and the proposed interventions to minimize its effects. Failure to address AMI is theorized to result in cortical reorganization, disability, decreased patient reported outcomes, and subsequent joint injury. Therefore, effective rehabilitation protocol should look to classify AMI & implement treatment specific interventions.
Purpose
The purpose of this presentation is to educate practicing physical therapy clinicians and students on the theoretical multi-faceted mechanism of Arthrogenic Muscle Inhibition, and provide meaningful interventions that may help reduce and/or prevent the potential effects of AMI from occurring. Thus, resulting in an increased potential improvement in patient-reported and clinical outcomes, and ultimately resulting in long-term rehabilitative success.
Products
My products for this capstone project include:
1. A DropBox Link To PowerPoint Presentation with an Included VoiceThread
2. A PDF Link to The Slides
https://acrobat.adobe.com/id/urn:aaid:sc:VA6C2:2486ce83-307d-44ba-b85c-4324b547c5ca
3. A PDF Containing An Audio Transcript Of the Recorded Slides
https://acrobat.adobe.com/id/urn:aaid:sc:VA6C2:91da2a5e-9639-47dc-810b-e4773fe9adf8
4. A Google Survey Evaluation Form
https://forms.gle/jZsrxKR9V5ki8uJf8
Self-Reflection
Overall, I enjoyed the time I spent learning about AMI and believe as though I have gained clinically important and useful information regarding the topic. However, the project was indeed more challenging than I originally expected when I chose the topic. The completion of this project required critical thinking and understanding of the interconnection between the musculoskeletal and neurological system. There were often times I felt unsure and defeated while working on the presentation. However, this project emphasized the importance of perseverance, and reaching out to colleagues for guidance. Additionally, from this project, I have enhanced my ability to critically analyze literature, and have refined my ability to prescribe patient specific interventions based on the patients current impairment(s). Ultimately, I am proud of the work I put into the project and am pleased with the final product.
Evaluation
Throughout the completion of the project, I presented two sub-sections of the final presentation to my lab group and received constructive feedback from my advisor, classmates, and lab members. In addition, after the mid-term draft was due, I began meeting with my advisor on a weekly basis. The feedback from the lab presentations and weekly meetings with my advisor, helped ensure the project both objectively flowed in a meaningful but concise manner and was aesthetically appealing.
Additionally, I created a google survey that is designed to provide feedback regarding how effective the presentation is as it relates to educating the audience on AMI and its clinical significance.
https://forms.gle/jZsrxKR9V5ki8uJf8
Acknowledgements
Louise Thoma, PT, DPT, PhD: You have made a profound impact on my academic career and I am extremely grateful that I have had the privilege of participating in the preceptorship. Throughout the school year you have always allowed for an open line of communication and have provided meaningful guidance that helped provide clarity and levelheadedness in situations where I felt uncertain. You have been a great mentor through and through! Thank you x10!!!
David Sherman, PhD, PT, ATC: I am extremely appreciative for your advice and insight throughout my completion of this project! You truly volunteered your time to provide guidance whenever it was desired. Your work and advice helped lay the foundation and guide this project! Thank you so much!
Sarah McAuliffe, PT, DPT: Thank you for taking the time to be a member of my capstone committee. I thoroughly appreciated my time with you in ICE, and believe that you are an extremely knowledgeable clinician who has helped guide my clinical knowledge and practice.
Carla Hill, PT, DPT, OCS, Cert MDT, CEEAA: I am thankful and very appreciative that you volunteered your time to participate on my capstone committee. Your feedback and guidance have been very valuable throughout the completion of this project.
UNC DPT CLASS OF 2023 FAMILY: I know it is a cliché saying but I literally cannot believe how fast 3 years have flown by. We started our PT journey as 29 strangers, learning separately across 4 different classrooms. However, we are leaving as a family that has genuinely enjoyed spending time with each other. I am extremely proud of each and everyone of you and I cannot wait to see and hear about all the continued success you all have in your careers!! UNC DPT CLASS of 2023, The Best Class To Ever Do It!!!
References
- Hopkins JT, Ingersoll CD. Arthrogenic Muscle inhibition: A Limiting Factor in Joint Rehabilitation. J Sport Rehabil. 2000;9(2):135-159. doi:10.1123/jsr.9.2.135
- Lepley AS, Lepley LK. Mechanisms of arthrogenic muscle inhibition. J Sport Rehabil. 2022;31(6):707-716. doi:10.1123/jsr.2020-0479
- Lepley AS, Bahhur NO, Murray AM, Pietrosimone BG. Quadriceps corticomotor excitability following an experimental knee joint effusion. Knee Surg Sports Traumatol Arthrosc. 2015;23(4):1010-1017. doi:10.1007/s00167-013-2816-1
- Rice DA, McNair PJ, Lewis GN, Dalbeth N. Quadriceps arthrogenic muscle inhibition: the effects of experimental knee joint effusion on motor cortex excitability. Arthritis Res Ther. 2014;16(6):502. Published 2014 Dec 10. doi:10.1186/s13075-014-0502-4
- Lewek M, Rudolph K, Axe M, Snyder-Mackler L. The effect of insufficient quadriceps strength on gait after anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon). 2002;17(1):56-63. doi:10.1016/s0268-0033(01)00097-3
- Pietrosimone B, Lepley AS, Kuenze C, et al. Arthrogenic muscle inhibition following anterior cruciate ligament injury. J Sport Rehabil. Published online February 14, 2022:1-13. doi:10.1123/jsr.2021-0128
- Palmieri-Smith RM, Thomas AC, Wojtys EM. Maximizing quadriceps strength after ACL reconstruction. Clin Sports Med. 2008;27(3):405-424, vii. doi:10.1016/j.csm.2008.02.001
- Palmieri-Smith RM, Thomas AC. A neuromuscular mechanism of posttraumatic osteoarthritis associated with ACL injury. Exerc Sport Sci Rev. 2009;37(3):147-153. doi:10.1097/JES.0b013e3181aa6669
- Sonnery-Cottet B, Hopper GP, Gousopoulos L, et al. Arthrogenic muscle inhibition following knee injury or surgery: pathophysiology, classification, and treatment. Video Journal of Sports Medicine. 2022;2(3):263502542210862. doi:10.1177/26350254221086295
- Sherman, PhD, DPT, ATC D. Formal Assessment of Arthrogenic Muscle Inhibition. September 27, 2022. Accessed February 20, 2023. https://www.live4pt.com/blog/formal-assessment-of-arthrogenic-muscle-inhibition