
Auditory Cues and Step Length during Treadmill Gait in Patients with Parkinson’s Disease
By: Guneet Chawla, SPT
Background
When it came time to think about Capstone projects, I knew that I wanted to do a research project. That desire led me to the opportunity to conduct this current research study with my co-principle investigator, Maddie Wygand, SPT, under the guidance of Dr. Mike Lewek, PT, PhD, My interest in investigating gait concepts in Parkinson’s Disease (PD) stems from my grandfather who had PD, as well as a patient I worked with during a clinical rotation last year. Through a literature review and conversations with Mike and Dr. Nina Browner, MD, we decided to study the effects of music and metronome cues on gait mechanics during over-ground and treadmill walking in patients with PD. The specific research question that I chose to focus on compares step length during different frequencies of metronome and music cues while walking on the treadmill.
Acknowledgments
Dr. Mike Lewek, PT, PhD – Your passion for research and mentoring students has been so evident to me during my time in the DPT program, and I really enjoyed the opportunity to complete this project under your guidance this year. This project would not have been possible without your enthusiasm, support, guidance, and expertise at every step of the way!
Dr. Nina Browner, MD – Thank you for your encouragement and guidance from the very beginning of this project, and for serving on my Capstone Committee! Your assistance with patient recruitment and expertise in Parkinson’s Disease was invaluable to designing and conducting this research study.
Diane Meyer, PT, MSCS – Thank you for serving on my Capstone Committee and providing me with feedback on manuscript in such a timely manner. I also appreciate your attendance at my presentation at the CRC. You provided important insight into the clinical implications of this research.
Maddie Wygand, SPT – I thoroughly enjoyed working with you on this research project and continue to be inspired by your passion, skillset, and determination. I couldn’t have asked for a better research partner!
Abstract
Background: Some of the common gait impairments in individuals with Parkinson’s Disease are forward trunk posture, postural instability, freezing episodes, and shuffled steps. Thus, gait training is an important component of rehabilitation for this population. Both music and metronome cues are used to improve gait, however there is no consensus on which is more effective. Furthermore, these cues are primarily applied to over-ground ambulation, and the effects on step length have been inconsistent.
Objective: To investigate the effect of metronome and music cues of various frequencies on step length during treadmill walking in patients with PD.
Methodology: Twenty-one individuals diagnosed with PD and classified as Hoehn & Yahr Stage I, II, or III participated in this single-session study. Baseline measurements were taken by having each participant walk across a Zeno pressure mat at their comfortable speed. Frequencies of auditory cues were calculated by taking 85%, 90%, 100%, and 115% of the individual’s comfortable cadence. Participants walked on a dual-belt treadmill at a constant speed for 1 minute under each of the following conditions: (1) no auditory cues, (2) Metronome at 85% of over-ground cadence, (3) Metronome at 90%, (4) Metronome at 100%, (5) Metronome at 115%, (6) Music at 85%, (7) Music at 90%, (8) Music at 100%, and (9) Music at 115%. Measures included step length (m), step length variability (m), and cadence (step/minute).
Results: Significant changes in step length on the treadmill were only seen with the metronome conditions. Music cues did not elicit any significant changes in step length. Longer step lengths was observed with 85% and 90% metronome conditions, while a shorter step length was observed with the 115% metronome condition. Appropriate changes in cadence were also observed, despite the actual cadences not matching the intended cadences.
Conclusion: Metronome is more effective than music at facilitating changes in step length on a treadmill. To produce longer step length in patients with PD, a treadmill at constant speed is an appropriate gait surface to use, while utilizing metronome cues at 85% or 90% of comfortable cadence.
Introduction:
Parkinson’s Disease (PD) is a progressive neurodegenerative disorder associated with decreased formation of dopamine in the substantia nigra of the basal ganglia1. It is the second most common neurodegenerative disorder2. The exact cause of PD remains unknown. Although some cases do appear to have a genetic component, the majority of cases remain idiopathic. Some of the typical symptoms that individuals with PD present with are tremor at rest, rigidity, bradykinesia, and postural instability. These symptoms result in a variety of functional impairments associated with gait and other forms of mobility. Some typical characteristics of gait in this population include flexed posture, shuffled steps, freezing episodes, and postural impairments. These impairments can result in increased falls risk due to their effects on balance and postural instability.1
Improvement of gait is a large focus of physical therapy treatment for patients with PD. In particular, facilitating longer step lengths to improve overall gait mechanics is considered beneficial due to the role of short, shuffled steps in the balance impairments and falls risk that manifests in this population3,4. One strategy that is often incorporated into rehabilitation is the use of rhythmic auditory stimulation (RAS), or auditory cues, to facilitate automaticity of gait5. The benefits of auditory cues on improving gait mechanics in this population have been well-documented, and previous studies have utilized both music and metronome as auditory cues to facilitate changes in gait4,6. A key benefit of a metronome is that the beat is discrete, and it enables greater synchronization between the individual’s steps and beat6,7. Although metronome cues have demonstrated some success in facilitating changes in gait velocity and cadence (steps/minute) in over-ground ambulation in the PD population, the effects on stride length have been mixed8,9. For instance, Picelli et.al. demonstrated that regardless of whether the metronome was slower or faster than comfortable cadence, stride length increased with cues compared to non-cued gait9. Howe et.al found that the stride length remained the same during all cued conditions, though velocity increased with faster frequencies and decreased with slower frequencies8. Many of these discrepancies can be attributed to testing over-ground, where speed can be changed.
Music represents another form of rhythmic auditory cuing and is commonly used during exercise. As individuals listen to music for auditory cueing, it can be more difficult to pick out the beat of a song and adjust gait to match it. There are often many layers of rhythms and beats embedded in music that make it continuous rather than discrete10. Nevertheless, a number of studies have looked at the effects of music on gait mechanics, and have found a generally favorable association between use of musical cues and increased stride length11,12,4,13. However, the cue frequencies at which this outcome was obtained varied greatly. Some individuals with PD have been found to produce longer strides with a frequency that is slower than their normal cadence11,12, while others were more successful at increasing stride length with cue frequencies faster than their normal cadence11,12,13. Additionally, these studies typically utilize musical tracks that have been specially designed for the research study and accentuate the rhythm so that it is easy to detect.
Comparisons between music and metronome cues are rarely performed. However, in studies involving healthy older adults, both music and metronome cues were effective in increasing cadence, but only musical cues significantly improved stride length and gait velocity14. Cueing from a metronome, however, was more effective in eliciting synchronization between steps and the auditory cues7.
These studies certainly highlight the ability to use auditory cues to improve gait in patients with PD, but no single study has compared the effects of music and metronome on gait in this population6. Furthermore, previous studies examining the use of auditory cues in the PD population have primarily included over-ground walking. When ambulating over-ground, individuals have the ability to change gait speed in response to the different frequencies of cuing, which is likely a contributing factor to why the effects on stride length are so varied across studies and individuals. Thus, we focused only on ambulation on a treadmill to carefully control gait speed. This design allows us to assess potential changes in step length across different conditions of auditory cues, while the treadmill speed remains constant. The purpose of this project is to determine the difference between metronome and music cues of various frequencies on step length during treadmill walking. Given the inability of individuals to change gait speed on the treadmill, we hypothesize that during exposure to cue frequencies slower than comfortable cadence, patients will be able to achieve target cadences to increase step length. We believe that the increase in step length will be particularly evident during conditions with metronome cues compared to the music cues due to the metronome rhythm being more distinguishable, promoting better synchronization between steps and auditory cues.
Methodology:
Procedures:
A sample of 21 individuals (ages 38-81; 13 males, 8 females) with a medical diagnosis of PD (Hoehn & Yahr I-III) agreed to participate in this study. Patients were recruited from the UNC Neurology Clinic and through local PD patient support groups. Participants who met the following criteria were included in this study: (1) self-reported ability to walk >10m over-ground, (2) self-reported ability to walk on treadmill for total of 14 minutes (with rest breaks as needed), and (3) classification of Stage I, II, or III on Hoehn and Yahr. Exclusion criteria include: Hoehn & Yahr Stage IV or V, uncontrolled cardiorespiratory or metabolic disease (i.e. uncontrolled hypertension, uncontrolled diabetes mellitus, orthostatic hypotension, chronic emphysema), other neurological or orthopedic disorders that may affect walking, severe communication or comprehension impairments that would impede ability to perform study procedures appropriately. All participants signed an informed consent form approved by the Institutional Review Board of UNC-Chapel Hill prior to participation.
All subjects participated in a two-hour testing session at the Interdisciplinary Human Movement Laboratory at the University of North Carolina – Chapel Hill. The Montreal Cognitive Assessment (MoCA) was administered to each subject at the beginning of the testing session to characterize cognitive deficits. An initial walk was performed over a 16 foot Zeno pressure mat (Prokinetics) to measure comfortable over ground gait speed and cadence without the presence of auditory cues. This gait speed was used to set the treadmill speed, while cadence was used to determine the four frequencies for auditory cues: 85%, 90%, 100%, and 115%. Each subject selected their own songs that matched the exact frequency for each condition from www.bpmdatabase.com.
We used a dual-belt treadmill (Bertec Corp, Columbus, OH) in this study. Prior to initiating testing on the treadmill, a single 14mm retro-reflective marker was taped to the posterior heel of each of the participant’s shoes. An 8-camera passive motion capture system (Vicon MX, Los Angeles, CA) sampling at 120 Hz was used to record the 3D location of both markers. Ground reaction forces were also measured using the treadmill’s force plates at 1200 Hz. These data were used to determine spatiotemoral parameters during gait. For safety purposes, each subject was placed in a harness that attached to the ceiling over the treadmill. The harness did not provide any body weight support, restrict limb motion, or change overall posture. Handrails were available on the sides of the treadmill and were utilized by 12 participants to increase stability during ambulation, though everyone was discouraged from using the handrails.
All subjects walked for 1 minute under each of the following 9 conditions on the treadmill: (1) no auditory cues, (2) Metronome at 85% of over-ground cadence, (3) Metronome at 90%, (4) Metronome at 100%, (5) Metronome at 115%, (6) Music at 85%, (7) Music at 90%, (8) Music at 100%, and (9) Music at 115%. Notably, participants selected different songs for each of the Music conditions to correspond with the different frequencies. This was necessary to play each song at its correct tempo, rather than artificially slowing down or speeding up a single song. Conditions were block randomized for each participant, first by type of auditory cue and then by frequency of cue. The condition with no auditory stimuli was always performed first, as it allowed patients to acclimate to walking on the dual-belt treadmill before proceeding to the cued trials. Auditory cues were played using Spotify or YouTube (for songs), and Google metronome. Participants were instructed to “step to the beat” of the music or metronome while the treadmill speed remained constant. Rest breaks were provided between conditions as needed. We monitored heart rate and oxygen saturation during treadmill walking using an ear clip and blood pressure before and after ambulation to ensure safety.
Data Processing & Outcome Measures
We looked at cadence, step length, and step length variability as the primary outcome measures of this study. A custom LabView program was used to calculate these outcomes. The program detected each heel strike where the vertical ground reaction force exceeded 20N. The time between each step was calculated and averaged over the total number of steps, and then the inverse of this value was used to obtain the cadence. Step length was calculated by measuring the anterior-posterior distance between the right and left heel markers at each heels strike. Step length variability was obtained by taking the standard deviation of step length averaged over the total walking time for each condition.
Data Analysis
Data analysis was performed using SPSS Version 24. Separate repeated measures Analysis of Variance tests (ANOVAs) repeated for condition were performed for each outcome measure. In the presence of significant main effects, we performed paired sample t-tests for post-hoc analyses. We accounted for multiple comparisons using Bonferroni corrections. P-values less than .05 were considered significant.
Results
Twenty-one subjects with PD participated in this study (13M/8F; age: 69.8 ± 9.81, MOCA score: 27.14 ± 2.92). With an average time since diagnosis of 8.33 ± 7.95 years, we recruited 5 with H&Y stage 1, 9 with stage 2, and 7 with stage 3. The average UPDRS score was 19.38 ± 13.65, with the average motor axial subscore being 4.8 ± 3.5. Nine participants were classified as axial rigid, while 12 were classified as tremor predominant. The average over-ground gait speed was 1.145 ± .206 and the average treadmill speed used for testing was 1.1 ± 0.26m/s.
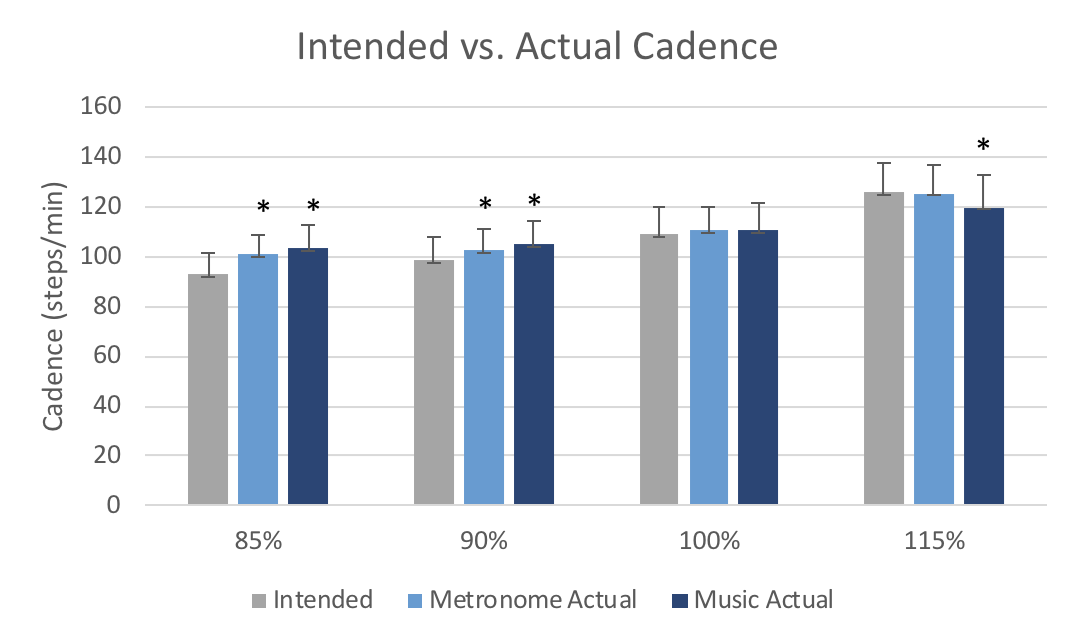
Participants were not able to achieve the intended cadence consistently (see Graph 1). Specifically, we observed a significantly higher actual cadence than what was intended for the following conditions: 85% Metronome (p<.001), 85% Music (p<.001), 90% Metronome (p=.004), and 90% Music (p=.001). Additionally, we observed a lower cadence than intended in the 115% Music condition (p=.007). Participants were able to successfully reproduce the intended cadence during the 100% metronome and music conditions (p>.39, = .042), and the 115% Metronome (p>.05) condition.
Graph 1: Comparison of intended and actual cadence by condition
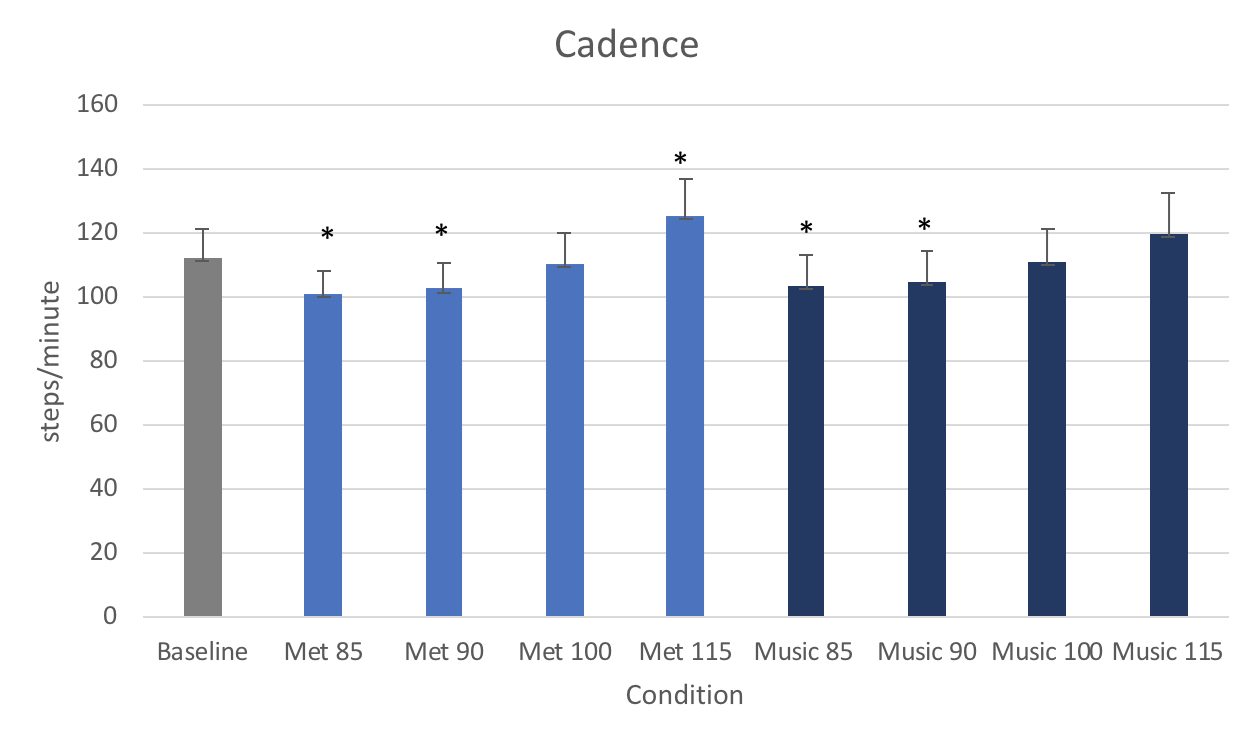
Nevertheless, we noted a significant difference in cadence across conditions (p<.001, = .946), as illustrated in Graph 2. Post hoc comparisons demonstrated significant decreases in cadence relative to baseline cadence for the 85% Metronome (p<.001), 90% Metronome (p<.001), 85% Music (p=.007), and 90% music (p<.007), while 115% metronome (p<.001) produced increased cadence. The cadence during 100% metronome (p>.05), 100% music (p>.05), and 115% music (p>.05) conditions did not significantly differ from baseline cadence.
Graph 2: Average cadence on treadmill across each condition
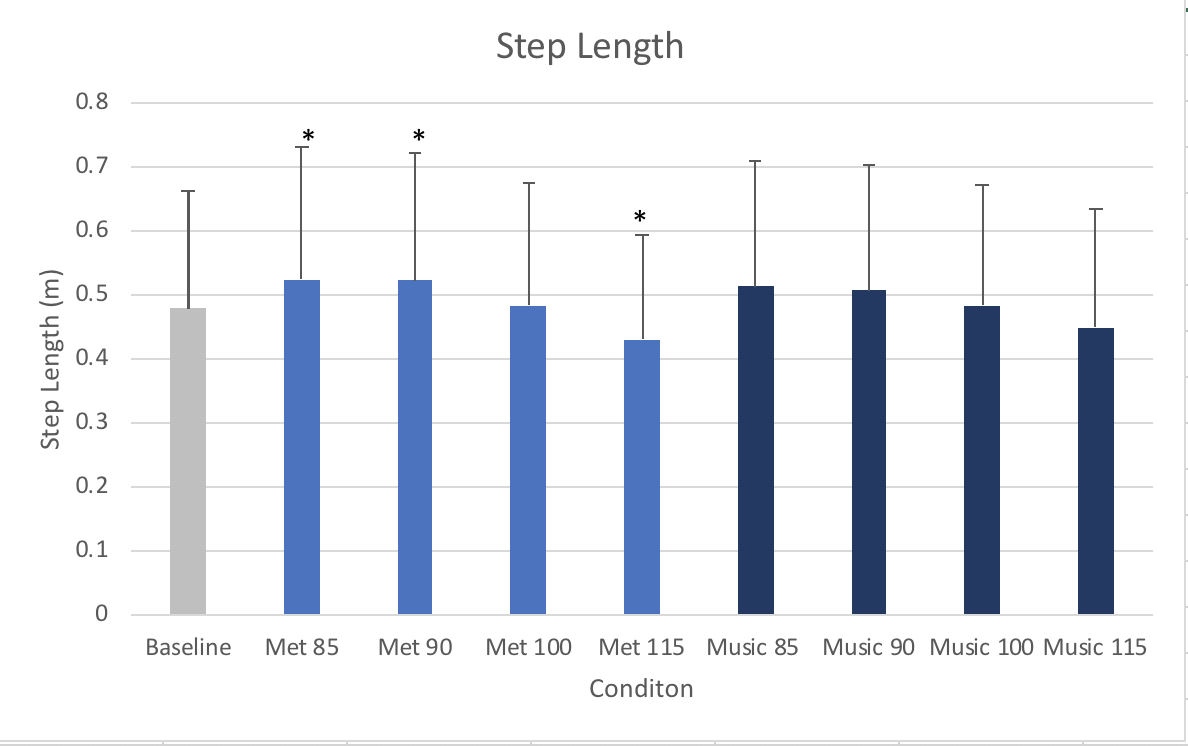
With regards to step length, a significant main effect was also found across conditions (p<.001, = .856) (see Graph 3). Specifically, longer steps were achieved during the 85% Metronome (p=.001) and 90% Metronome (p=.002) conditions, whereas the 115% Metronome (p=.002) produced significantly shorter step lengths. None of the conditions utilizing music cues produced significant changes to step length (p>.05). Additionally, we observed no significant main effect for step length variability across conditions (p>.05, = .068)
Graph 3: Average step length on treadmill across each condition
Discussion
Our hypothesis that metronome cues would elicit a greater response than music were supported by the data. Likewise, our hypothesis that cues at a frequency slower than comfortable cadence will produce greater step length on the treadmill was supported. Results found that both 85% and 90% frequency cues produced a step length significantly greater than that at baseline, despite the steps not matching the intended cadence. These findings have implications for identifying parameters of auditory cues that are effective for facilitating longer step length in patients with PD during treadmill ambulation.
Previously, some researchers have suggested that the continuity of music requires less cognitive demand than cues that have a fixed beat, such as a metronome6. Furthermore, previous studies have found musical cues to be associated with improvement in gait speed, cadence, and stride length 11–13,15. In our study however, only the metronome was able to elicit significant changes in step length on the treadmill, whereas music was not. Subjective comments from participants revealed sentiments consistent with this finding, in that most individuals reported greater ease in identifying the tempo during metronome cues versus the music cues. The differences between the current findings and prior work can largely be attributed to the variation in ambulation surface and type of songs used to provide cues. Prior research has looked at ambulation over ground11–13,15, whereas our study was done on the treadmill to eliminate the confounding effect of gait speed changes. Additionally, studies up until now have primarily used musical tracks that have been artificially altered or specifically designed to highlight the beat of the music and enable people to easily detect rhythm. However, this is not always feasible to implement in the clinical or community setting, which is why we opted to use publicly available music.
We also found that on the treadmill, utilizing a metronome or music cue frequency that is slower (i.e., 85% or 90%) than the individual’s comfortable cadence facilitates a longer step length, whereas faster cues (115%) lead to a shorter step length. This finding is in contrast to previous studies conducted over-ground that found that even cues faster than a person’s comfortable cadence can produce increased stride length9, or that stride length remained the same despite the cue frequency8. The ability of an individual to change gait speed over-ground is certainly a contributing factor to that variable findings. The results of our study demonstrate that when speed is being controlled on the treadmill, people with PD are in fact able to take longer steps with exposure to metronome cues at frequencies slower than their comfortable cadence.
For purposes of applying these findings to PD rehabilitation, it is noteworthy that the increases in step length were observed with lower metronome cue frequencies despite the subjects not being able to completely synchronize their steps to the beat. Research involving healthy subjects has found that the ability to synchronize steps to rhythmic auditory stimuli is improved with faster music and music that the individual is familiar with7,16. On the other hand, synchronization between gait and auditory cues does not seem to be a major focus of previous research conducted with the PD population13. In our study, neither the metronome nor music conditions were able to produce exact synchronization between steps and cues. Yet, there were still significant effects observed for step length.
A potential limitation of our study is that some subjects held onto the rails while completing the walking trials on the treadmill. Although we encouraged the patients to not hold the rails, many of them felt more stable while holding them. All individuals who chose to use handrails during the study held onto them consistently across the conditions. Research involving individuals following stroke demonstrates that holding the handrails on the treadmill results longer step length and greater step length symmetry17. Thus, it is reasonable to suspect some potential skewing of the step length data caused by holding onto handrails. It is also possible that handrail use contributed to the consistency in step length that we found, resulting in no differences in step length variability between the various cuing frequencies.
There was no specific protocol regarding rest breaks during the testing, except that they would be provided in between conditions whenever the patient asked for one. As a result, each participant took a different number of rest breaks. Fatigue can alter gait mechanics by decreasing step length and increasing trunk sway, step width, and step length variability18. Although participants were instructed to ask for a rest break whenever they needed one, it is likely that each individual experienced different levels of fatigue during the testing, and was affected differently by factor.
Another limitation is the song selection. Each participant had different songs, and some songs may have started in a place where the beat was difficult to distinguish. This would have been a difficult variable to control, given that the intended study design was to allow participants to select types of songs that are publicly available and that they hopefully enjoy.
Lastly, we were unable to recruit the same number of participants for each Hoen and Yarber Scale I-III due to the pool of individuals that expressed desire to participate in this study. This resulted in a greater number of patients classified as Stage 2 or 3, rather than Stage 1. This may have led to presentations and gait parameters more consistent with someone who has a slightly more advanced stage of PD.
This study focused on the immediate effects of different auditory cue types and frequencies on spatiotemporal gait parameters during treadmill ambulation. Further research could be conducted to assess long term outcomes of treadmill training with 85% or 90% metronome cues on step length, and whether the effects would carry over to over-ground ambulation.
Shorter steps are a key characteristic of parkinsonian gait, and can lead to decreased balance, postural instability, and increased falls risk3,4. Our study demonstrates that a treadmill at constant speed is an appropriate gait surface to use for facilitating longer step lengths in patients with PD. Although subjects were unable to fully synchronize their steps to the slower metronome cues, they were still able to significantly reduce their cadence, as well as take significantly longer steps.
Bibliography
- Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatr 2008;79(4):368-376. doi:10.1136/jnnp.2007.131045.
- de Lau LML, Breteler MMB. Epidemiology of Parkinson’s disease. Lancet Neurol 2006;5(6):525-535. doi:10.1016/S1474-4422(06)70471-9.
- Morris ME, Martin CL, Schenkman ML. Striding out with Parkinson disease: evidence-based physical therapy for gait disorders. Phys Ther 2010;90(2):280-288. doi:10.2522/ptj.20090091.
- Spaulding SJ, Barber B, Colby M, Cormack B, Mick T, Jenkins ME. Cueing and gait improvement among people with Parkinson’s disease: a meta-analysis. Arch Phys Med Rehabil 2013;94(3):562-570. doi:10.1016/j.apmr.2012.10.026.
- Keus SHJ, Munneke M, Nijkrake MJ, Kwakkel G, Bloem BR. Physical therapy in Parkinson’s disease: evolution and future challenges. Mov Disord 2009;24(1):1-14. doi:10.1002/mds.22141.
- Ashoori A, Eagleman DM, Jankovic J. Effects of auditory rhythm and music on gait disturbances in parkinson’s disease. Front Neurol 2015;6:234. doi:10.3389/fneur.2015.00234.
- Leow L-A, Parrott T, Grahn JA. Individual differences in beat perception affect gait responses to low- and high-groove music. Front Hum Neurosci 2014;8:811. doi:10.3389/fnhum.2014.00811.
- Howe TE, Lövgreen B, Cody FWJ, Ashton VJ, Oldham JA. Auditory cues can modify the gait of persons with early-stage Parkinson’s disease: a method for enhancing parkinsonian walking performance? Clin Rehabil 2003;17(4):363-367. doi:10.1191/0269215503cr621oa.
- Picelli A, Camin M, Tinazzi M, et al. Three-dimensional motion analysis of the effects of auditory cueing on gait pattern in patients with Parkinson’s disease: a preliminary investigation. Neurol Sci 2010;31(4):423-430. doi:10.1007/s10072-010-0228-2.
- Rodger MWM, Craig CM. Beyond the Metronome: Auditory Events and Music May Afford More than Just Interval Durations as Gait Cues in Parkinson’s Disease. Front Neurosci 2016;10:272. doi:10.3389/fnins.2016.00272.
- Benoit C-E, Dalla Bella S, Farrugia N, Obrig H, Mainka S, Kotz SA. Musically cued gait-training improves both perceptual and motor timing in Parkinson’s disease. Front Hum Neurosci 2014;8:494. doi:10.3389/fnhum.2014.00494.
- Bella SD, Benoit C-E, Farrugia N, et al. Gait improvement via rhythmic stimulation in Parkinson’s disease is linked to rhythmic skills. Sci Rep 2017;7:42005. doi:10.1038/srep42005.
- Ford MP, Malone LA, Nyikos I, Yelisetty R, Bickel CS. Gait training with progressive external auditory cueing in persons with Parkinson’s disease. Arch Phys Med Rehabil 2010;91(8):1255-1261. doi:10.1016/j.apmr.2010.04.012.
- Wittwer JE, Webster KE, Hill K. Music and metronome cues produce different effects on gait spatiotemporal measures but not gait variability in healthy older adults. Gait Posture 2013;37(2):219-222. doi:10.1016/j.gaitpost.2012.07.006.
- Thaut MH, McIntosh GC, Rice RR, Miller RA, Rathbun J, Brault JM. Rhythmic auditory stimulation in gait training for Parkinson’s disease patients. Mov Disord 1996;11(2):193-200. doi:10.1002/mds.870110213.
- Leow L-A, Rinchon C, Grahn J. Familiarity with music increases walking speed in rhythmic auditory cuing. Ann N Y Acad Sci 2015;1337:53-61. doi:10.1111/nyas.12658.
- IJmker T, Lamoth CJ, Houdijk H, et al. Effects of handrail hold and light touch on energetics, step parameters, and neuromuscular activity during walking after stroke. J Neuroeng Rehabil 2015;12:70. doi:10.1186/s12984-015-0051-3.
- Helbostad JL, Leirfall S, Moe-Nilssen R, Sletvold O. Physical fatigue affects gait characteristics in older persons. J Gerontol A Biol Sci Med Sci 2007;62(9):1010-1015. doi:10.1093/gerona/62.9.1010.
3 Responses to “Auditory Cues and Step Length during Treadmill Gait in Patients with Parkinson’s Disease”
Michael Lewek
Guneet,
You did such a nice job on this project. I’ve already drafted a follow-up study to submit as a pre-proposal to the Michael J Fox Foundation. It really was a pleasure to work with you this year.
Mike
Guneet Chawla
Hi Alan! Thanks for your comments! So I did not look into any specific literature that compared community ambulation to clinic ambulation in this population, but if I do find anything I will send it your way!
With regards to solid ground versus clinic treadmill – none of the existing literature really looked at this comparison. Which was part of the basis for our project. So if you put together Maddie’s capstone and my capstone, the ultimate message is that for changing step length, treadmill is more effective than over ground – because on the ground individuals end up adjusting their gait speed, and their step length across conditions stays essentially the same.
The next step of our research would certainly be to see how it translates into a training program, and then ultimately how to apply it to the community.
Thanks for your question, and I hope this helps some!
Alan Levinson
Hello Guneet,
Your capstone research project is very interesting. I enjoyed your presentation of the project earlier this week at the CRC.
You describe a fairly long list of variables, (metronome v. music; 4 different percentages of “comfortable cadence) and clearly explained the relationships among all conditions and effect on step length. Well done!
I was somewhat surprised to learn that while there is some literature support for use of music to provide auditory rhythmic cues for gait training, your research showed that use of a metronome is statistically and significantly more effective in improving step length for patients with PD.
Did you come across any literature that assesses effectiveness of metronome for improving step length in the community or on solid ground versus the clinic treadmill? Translating research findings to community application has been top of mind for me over the past semester.