
The Role of Terrain on Gait Speed and Spatiotemporal Measures
Stacy Harris, SPT
During one of my clinical rotations in the UNC Physical Therapy program, I experienced providing care in the home health setting. Treating individuals recovering in their own homes was an enlightening experience. It gave me the opportunity to train them on the terrains surrounding their homes, helping them to improve their ability to navigate their environment. This experience inspired me such that I hope to be able to work in this setting at some point in my career. It also led me to participate in a research elective in Fall 2017, where we studied the potential changes in gait that occur from walking during an indoor 10 Meter Walk Test to walking on various outdoor terrains. My hope was that I might gain some insight into how to better train patients for community ambulation, with the goal of improving their ability to participate in community activities.
My capstone project includes a manuscript outlining the study, our results, and implications for therapy treatment. Additionally, we gave a presentation of our results at the UNC Center for Rehabilitation Care, the location where we conducted our research. In the future, we plan to submit a more complete manuscript for publication following additional data analysis and feedback on our capstone projects. Finally, last semester alongside my research elective I completed a critically appraised topic to find the best evidence currently available regarding ways to improve gait speed in patients following stroke.
My capstone project was made possible with the guidance of Dr. Michael Lewek, PT, PhD, support of my research partner Alan Levinson, SPT, and the assistance of Catherine “CJ” Hamilton, PT, MSCS and all of the physical therapists at the UNC Center for Rehabilitation Care. Additionally, I would like to thank Catherine “CJ” Hamilton, PT, MSCS and Mary Moutoux, PT, MS, GCS for being willing to serve on my committee and provide feedback on my work.
Abstract
Background: Gait speed is used to predict health status and disability. Gait speed and its underlying spatiotemporal measures have been studied on level clinic surfaces and outdoor firm surfaces. However, the change in gait speed that occurs from a smooth, firm clinic setting to various outdoor terrains an individual may encounter in the community has not been studied.
Methods: Average gait speed, step length, and cadence were determined for 49 participants on the indoor 10 Meter Walk Test and six outdoor terrains: large pavers, sand, up and downhill gravel, mulch, and small pavers. Outcome measures were compared between conditions using a one-way repeated measures ANOVA, repeated for terrain. To determine the relationship between gait speed changes and both cadence and step length changes across conditions we used step-wise, multiple linear regression.
Results: There was a significant main effect across all terrains for gait speed (p < 0.001; ηp2 = 0.644), cadence (p < 0.001; ηp2 = 0.323), and step length (p < 0.001; ηp2 = 0.597). Gait speed was significantly slower on sand, mulch, and going up and downhill on gravel (all p < 0.023). Cadence and step length were significantly reduced on sand and going up and downhill on gravel (all p < 0.006 and p < 0.017, respectively). A combination of step length and cadence changes accounted for >94% of the variance in gait speed change from the 10MWT to sand speed (p < 0.001, R2 = 0.938), mulch speed (p < 0.001, R2 = 0.962), downhill gravel speed (p < 0.001, R2 = 0.937), and uphill gravel speed (p < 0.001, R2 = 0.938).
Conclusion: Indoor gait speed during a 10MWT is not representative of the speed individuals will use when walking on various outdoor terrains. Reduction in both step length and cadence results in this reduction in gait speed. Gait training should take place on the terrains individuals are expected to encounter upon reentering the community.
Introduction
A primary role of physical therapists is to restore independent mobility in the community for patients who have deficits with balance and mobility impairments. Improving gait is often listed as a primary goal of both patients1 and therapists, indicating its importance for physical functioning and quality of life. As such it is critical that therapists are able to objectively measure gait outcomes to ascertain their importance for community functioning. In particular, physical therapists frequently use the measure of gait speed in clinical settings, as it has previously been found to be a reliable predictor of health status and disability.2–4 In addition, decreased gait speed can lead to reduced participation in community activities as well as increased safety concerns, particularly in urban areas.5,6
A number of injuries and disabilities can cause mobility deficits leading to decreased gait speed, such as hip fracture, stroke, and spinal cord injury.4,7–9 Normative values have been established for gait speed using the 10 meter walk test in healthy adults to use as a comparison for people with mobility deficits.10 Additionally, cut off scores have been defined that are used to classify a person’s ambulation status, with lower speeds predictive of household and limited community ambulation and higher speeds predictive of unlimited community ambulation ability.3,11
Importantly, however, these norms and cut off scores were derived from measures taken in clinical settings that are well lit, indoors, and over a clear, flat surface. Instead, walking in the ‘real world’ is not simulated in this environment and is therefore not indicative of how individuals with mobility deficits might be actually walking in the community. In particular, people seldom walk on smooth, well-lit floors once they venture out of their homes. Instead, we must contend with various slopes and surface textures. These textures include different surface stiffnesses and as such have different requirements for balance and dynamic stability.12 Because patients seeking physical therapy for mobility deficits often present with balance deficits, it is likely that a transition to such terrains would require adaptations in gait speed to compensate.
Gait speed is affected by changes in spatiotemporal measures, which include step length and cadence.13,14 Typically, gait speed is increased by increasing step length and also increasing cadence,13,14 and step length and/or cadence is understood to change with age,14 on varying surface stiffnesses,12 and with various mobility impairments, such as Parkinson’s disease.15 For example, decreases in gait speed of older adults is mainly attributed to a reduction in step length, while cadence remains largely similar with only minor reduction.14,16 Walking on up- or down-sloped surfaces, also has an effect on step length and cadence. When walking downhill, step length tends to decrease more as the angle of the slope is increased, while walking uphill causes a reduction in step length, cadence, and gait speed that is also greater as the angle of the slope increases.17
There are many studies that define the characteristics of gait, gait speed, and its underlying spatiotemporal measures on level clinic surfaces or outdoor firm surfaces, however, few studies have addressed ambulation over varying terrains and, to our knowledge, there are no studies that compare indoor clinic gait speed to outdoor, community settings with typical community terrain obstacles such as gravel, mulch, slopes, etc. for people with mobility deficits.5,18–20 It is therefore important to understand how our measures of gait obtained on a smooth, firm standard floor translate to other typically encountered terrains in the community.
The purpose of this project was to quantify the change in gait speed that occurs from a smooth, firm clinic setting to various outdoor terrains that a patient may encounter in the community such as pavers, sand, upward and downward sloping gravel, and mulch. Our hypothesis is that the participants’ gait speed, obtained via the 10 Meter Walk Test in the clinic, will be reduced when traversing the various outdoor terrains. If this is the case, we aim to ascertain which spatiotemporal mechanism, cadence and/or step length, contributes to this change in gait speed so that instruction can be tailored in a manner that best supports restoration of gait speed and safe re-entry into the community.
Methods
Participants
We recruited 49 participants with mobility deficits due to musculoskeletal or neurological deficits. All participants were recruited at the site of the data collection via identification from their physical therapist. To be included in the study, the participants were required to ambulate with contact guard assist (CGA) or less, with or without an assistive device and/or orthotic, and were restricted to the age of 18 or older. Participants with comorbidities, such as partial blindness or dementia, were not excluded; two participants who spoke Spanish participated with the assistance of an interpreter. All participants signed an informed consent form approved by the IRB at the University of North Carolina at Chapel Hill.
Data Collection
Data collection occurred at the UNC Center for Rehabilitative Care in the therapy gym, and on their outdoor ‘Challenge course’. Participants were recorded with a standard video camera completing the 10 Meter Walk Test (10MWT) indoors and covering all parts of the Challenge course in the same order. One investigator reviewed consent paperwork with each participant, provided instructions on the 10MWT and outdoor course, and walked behind all participants to provide hand signals indicating when they were in line with the course markers. The second investigator collected demographic, subjective, and objective information, and captured video of all participants during indoor and outdoor testing. Participants who ambulated with contact guard assistance were guarded by their physical therapist, while participants who ambulated independently were usually unaccompanied.
The 10MWT was conducted indoors on a linoleum floor, in a well-lit corridor free of obstacles. The start and finish markers were on the floor in the form of blue tape, however participants were instructed to disregard those marks. Participants were allowed to use an assistive device, prosthetic, and/or orthotic, as needed. Prior to beginning the test, participants were instructed to stand about 2 meters behind the first marker to provide an acceleration zone. The instructions given were, “When I say ‘start,’ I would like for you to walk all the way to the opposite wall at a pace that is comfortable and safe for you.” The finish marker was several feet away from the opposite wall, so once the participant had passed over the marker they could safely decelerate. In most cases the 10MWT was conducted prior to the outdoor course, with a few exceptions due to time constraints surrounding the participant’s appointment time.
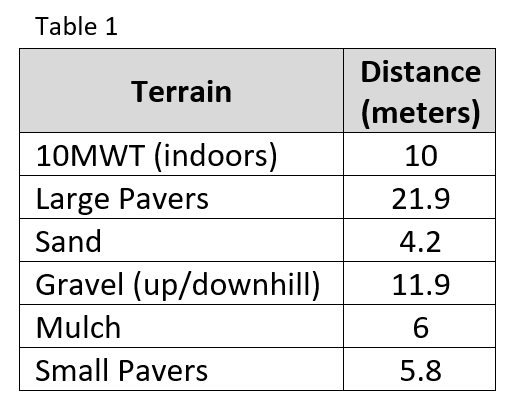
The participants were asked to make one clockwise and one counter-clockwise loop around the outdoor course. In the clockwise direction, the course consists of five varied terrains: large cement pavers, sand, downhill sloping gravel, mulch, and small cement pavers [see Table 1 for path distances]. Distances of each terrain were measured with a measuring wheel and flags were posted as markers to be visible on the videos. In the counter-clockwise direction, participants navigated the same terrains in reverse, resulting in the gravel terrain being sloped upwards. Participants were instructed to use the same assistive device, prosthetic, and/or orthotic that was used on the indoor 10MWT. The same verbal instructions were given regarding ambulating on the outdoor course, “I would like for you to walk around the course at a pace that is comfortable and safe for you.” Verbal and visual cueing was used while on the course to direct participants to the next terrain. Between the two loops, participants were allowed to take a standing, propped, or seated rest for up to 5 minutes, if requested.
Data Processing
Video clips of participants were downloaded to a standard PC and processed by the two investigators and a lab assistant. Data processing started by counting steps and recording start and finish times for each terrain, to the nearest tenth of a second. For every terrain (including the indoor 10MWT) the time began and ended when the participant’s torso was in line with the marker (or flag). When counting the number of steps, the first step where the foot was more than halfway past the marker was counted (heel or completely past). Step were counted until the last step prior to the final marker. If the last step was in line with the marker, it was only counted if the foot was less than halfway past (toes/forefoot) the marker. If the participant stopped on the course, the time was not stopped and step counting resumed when they began to ambulate again. When fully visible in the video, the markers laid out indoors and on the outdoor course were used to establish start and finish points; however, when not easily viewable the investigator’s hand signal was used as a guide. The time each participant required to navigate each terrain was calculated and used along with the distance and the number of steps on the terrain to calculate the participant’s average gait speed (distance/time), cadence (steps/time), and step length (distance/steps).
Data Analysis
Data analysis was performed in SPSS v24. Each of the outcome measures (gait speed, cadence, step length) were compared between conditions using a one-way repeated measures ANOVA, repeated for terrain. In the presence of significant main effects, we used paired samples T-tests as post-hoc tests. Multiple comparisons were accounted for using Bonferroni corrections. To determine the relationship between gait speed changes and both cadence and step length changes across conditions we used step-wise, multiple linear regression. P values less than 0.05 were considered significant.
Results
There were 50 interested participants who signed the informed consent form and completed the 10MWT, however, one participant was excluded from data analysis because she was unable to complete any outdoor terrain segments due to extreme fatigue. Of the 49 people included in the data analysis, there were 22 males and the average age of all participants was 65.2 + 15.8 years old (range from 23.1 to 86.4 years old). Participant diagnoses included 11 with Parkinson’s disease, 8 recovering from stroke, 19 with musculoskeletal complaints (arthritis, amputation, pain, etc.), 4 who suffered trauma (traumatic brain injury, spinal cord injury, pain due to motor vehicle crash injury), and 7 other conditions (spina bifida, cancer related pain, falls prevention, multiple sclerosis, shortness of breath with weakness). There were eight participants who used a cane (one of those had a knee brace), two participants utilized a Bioness, two wore ankle braces, one wore an ankle foot orthotic, one used a trans-femoral prosthetic, one used bilateral trans-tibial prosthetics, and one participant had a shoe lift. Twenty-three participants reported a history of falls. Of those reporting falls, the number reported ranged from 1 to 12 within the past year, with an average number of 2.4 falls for each faller.
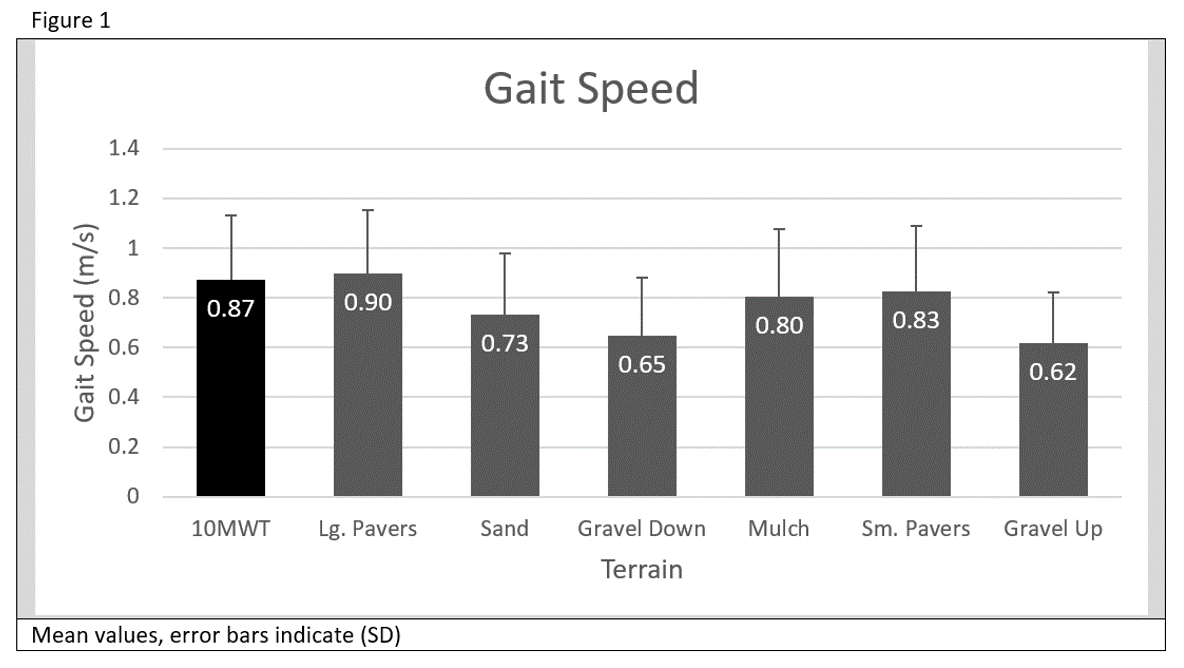
We observed a significant main effect for gait speed across the different walking terrains (p < 0.001; ηp2 = 0.644). Specifically, we noted that subjects walked significantly slower on sand, mulch, and going up and downhill on gravel (all p < 0.023). Both large and small pavers did not produce a significant change in speed. [see Figure 1]
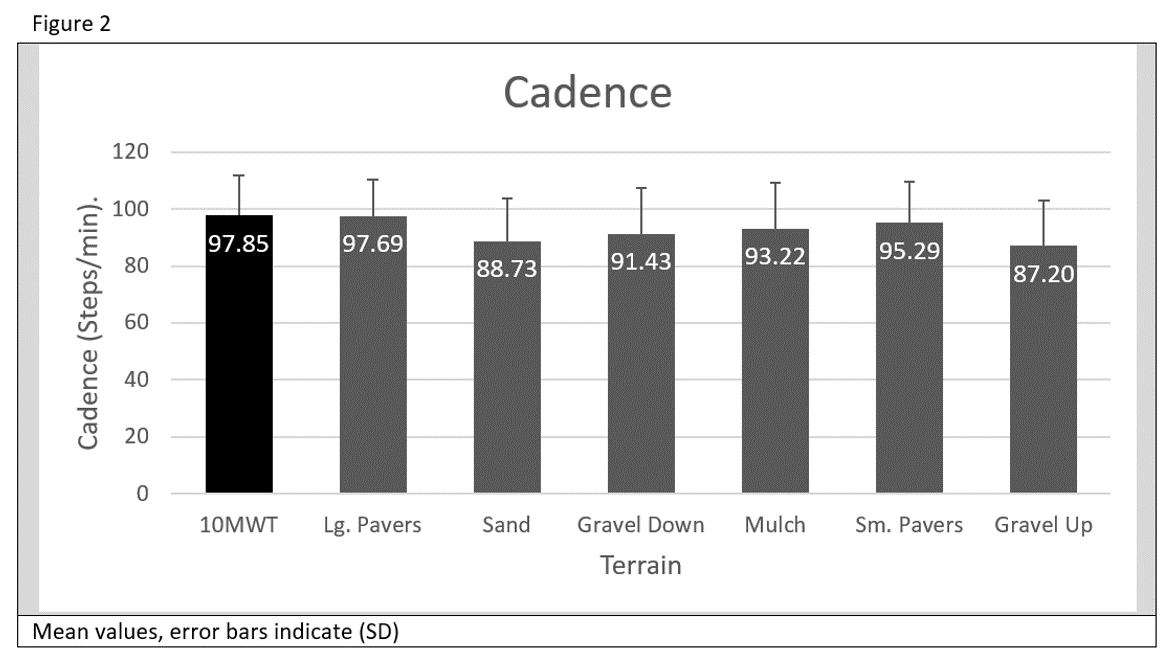
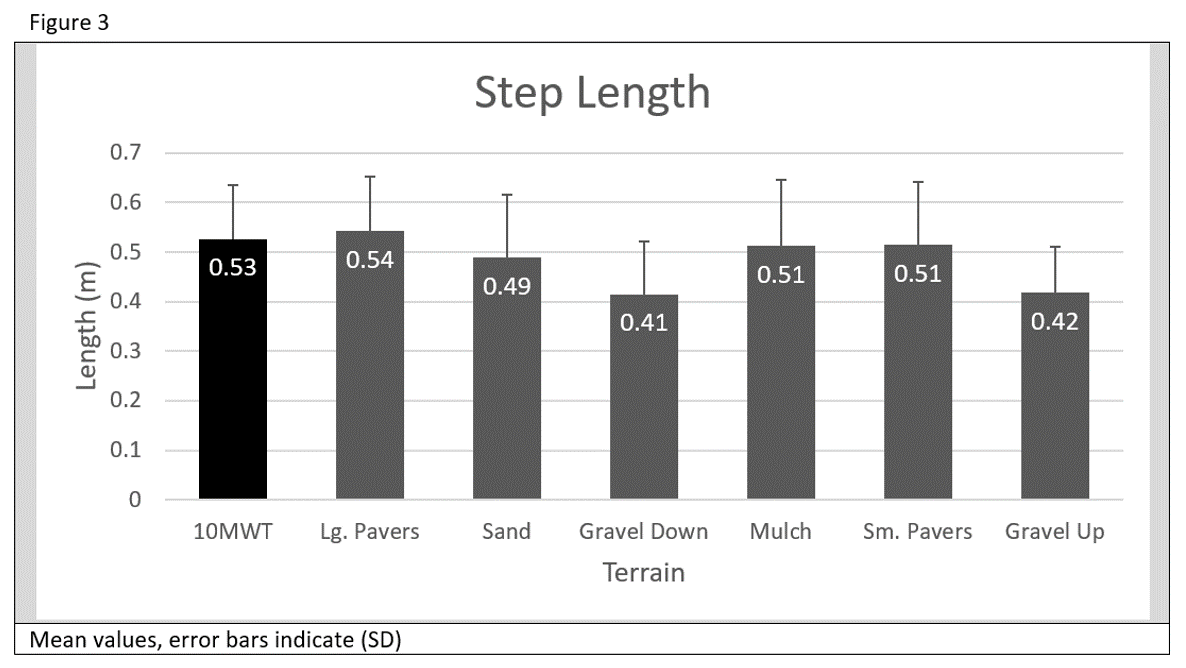
We also observed a significant main effect for cadence (p < 0.001; ηp2 = 0.323), as well as step length (p < 0.001; ηp2 = 0.597), across the different walking terrains. We noted that the cadence and step length of the subjects was significantly reduced on sand and going up and downhill on gravel (all p < 0.006 and p < 0.017, respectively). Neither mulch nor large or small pavers produced a significant change in cadence or step length. [see Figure 2 and 3]
The change in gait speed was significantly related to the combination of change in step length and change in cadence going from the 10MWT condition to the sand, mulch, and up and downhill gravel conditions. Specifically, we observed that the combination of step length and cadence changes accounted for 94% of the variance in gait speed change from the 10MWT speed to the sand speed (p < 0.001, R2 = 0.938), 96% of the variance in gait speed change from the 10MWT speed to the mulch speed (p < 0.001, R2 = 0.962), 94% of the variance in gait speed change from the 10MWT speed to the downhill gravel speed (p < 0.001, R2 = 0.937), and 94% of the variance in gait speed change from the 10MWT speed to the uphill gravel speed (p < 0.001, R2 = 0.938).
(Click each image to enlarge)
Discussion
Our hypothesis that the participants’ gait speed, obtained via the 10MWT in the clinic, would be reduced when traversing the various outdoor terrains was partially supported by the data. There was a reduction in gait speed when walking on sand, mulch, and walking up and downhill on gravel, although there was no change in gait speed walking on large or small pavers. With regard to the spatiotemporal measures of step length and cadence, both were reduced when walking on sand and up and downhill on gravel. It was determined that both the reduction in step length and reduction in cadence were concurrently responsible for the reduction of speed on the aforementioned terrains. This has important implications for individuals who wish to resume walking on outdoor terrains.
Our results have the potential to influence the structure of physical therapy treatments. Previous literature has suggested that patients with mobility deficits, such as stroke, are more likely to achieve the step quantity needed for limited community ambulation if their gait speed in the clinic is greater than 0.49 m/s, and are more likely to be able to achieve the step quantity needed for unlimited community ambulation if their gait speed is at least 0.93 m/s.11 The mean gait speed of our participants was 0.87 m/s on the 10MWT. Based on these values, the majority of our participants are most likely considered limited community ambulators, however the mean gait speeds on sand, mulch, uphill gravel, and downhill gravel were 0.73 m/s, 0.80 m/s, 0.62 m/s, and 0.65 m/s, respectively. Although they may be capable of some aspects of community ambulation, this reduction in speed may indicate that the participants are not ready for the increased demand those terrains require. Additionally, as average comfortable gait speed for healthy adults in the age range of our participants’ is between 1.27 and 1.46 m/s,10 this difference is a noteworthy indication of their ability to keep up with their peers in everyday life. It is clear that using these guidelines for discharge planning are not sufficient, and to truly prepare our patients for community ambulation and participation we should be training and testing them on the types of terrains they will be expected to traverse following discharge.
Navigating compliant terrains, like those in our study, requires greater amounts of dynamic stability.12 Importantly, gait differed from the indoor 10MWT only when participants walked on unstable surfaces (i.e. sand, much, gravel hills), but not on the stable outdoor surfaces (i.e. pavers). Under unimpaired conditions, step length will increase on compliant unstable surfaces to help increase the base of support.12 Therefore, it is important not only to gait train our patients on these surfaces, but also to focus on the cause of the reduction in gait speed – reduced step length and reduced cadence. This information should be used when informing instructional cues during gait training, as well as incorporating usual exercises and activities into therapy for increasing lower extremity strength and dynamic balance.
There were some limitations to our study. First, we did not formally track which participants had been on the outdoor Challenge course prior to our observations. It is possible that those that had been on the course previously would not have shown as much of a difference in walking speed outdoors due to their training. If anything, based on our results, we believe that if we had limited our study only to participants who had not yet been on the course, the difference in mean gait speeds might have been larger. Secondly, it is possible that the pace of the therapist and/or investigator could have unintentionally influenced the participant’s speed on the course. However, given that some participants required CGA or close guarding for safety, this seems to be an unavoidable limitation. Finally, we did not have a control group of unimpaired participants to compare against our results. Nevertheless, in comparing the participants’ mean gait speed on the various terrains against their own indoor 10MWT mean gait speed, we believe that the information we gained still has clinical significance to the practice of physical therapy.
One strength of our study is the variety of patient populations included in the study. This allows our results to be generalizable to the treatment of a broader range of mobility deficits. In addition, the use of a video recorder and verification (i.e. flags, landmarks, and hand signals) of start and finish lines for each outdoor terrain path contribute to the accuracy and precision of the data collected. These procedures allowed for less possibility of human error in counting steps and recording times as well as the ability of the video clip to be reviewed by more than one investigator for clarification.
Future research may include an assessment of training on various types of outdoor terrains to determine influence of such training on gait over uneven terrains. Such information would provide important information about the best method(s) for more complete rehabilitation of patients with mobility deficits.
Conclusion
The gait speed of patients observed indoors during a 10MWT is not representative of the speed they will use when walking on various outdoor terrains. Their reduction in gait speed is a result of a reduction in both step length and cadence. Physical therapists should be training patients on the terrains they expect them to encounter once they reenter the community along with other interventions targeting dynamic balance and strength.
Resources
- Bohannon RW, Andrews AW, Smith MB. Rehabilitation goals of patients with hemiplegia. International Journal of Rehabilitation Research 1988;11(2):181-184. doi:10.1097/00004356-198806000-00012.
- Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci 2000;55(4):M221-31.
- Bowden MG, Balasubramanian CK, Behrman AL, Kautz SA. Validation of a speed-based classification system using quantitative measures of walking performance poststroke. Neurorehabil Neural Repair 2008;22(6):672-675. doi:10.1177/1545968308318837.
- Chui KK, Lusardi MM. Spatial and temporal parameters of self-selected and fast walking speeds in healthy community-living adults aged 72-98 years. J Geriatr Phys Ther 2010;33(4):173-183.
- Shumway-Cook A, Patla AE, Stewart A, Ferrucci L, Ciol MA, Guralnik JM. Environmental demands associated with community mobility in older adults with and without mobility disabilities. Phys Ther 2002;82(7):670-681.
- Eggenberger P, Tomovic S, Münzer T, de Bruin ED. Older adults must hurry at pedestrian lights! A cross-sectional analysis of preferred and fast walking speed under single- and dual-task conditions. PLoS ONE 2017;12(7):e0182180. doi:10.1371/journal.pone.0182180.
- Hollman JH, Beckman BA, Brandt RA, Merriwether EN, Williams RT, Nordrum JT. Minimum detectable change in gait velocity during acute rehabilitation following hip fracture. J Geriatr Phys Ther 2008;31(2):53-56.
- Severinsen K, Jakobsen JK, Overgaard K, Andersen H. Normalized muscle strength, aerobic capacity, and walking performance in chronic stroke: a population-based study on the potential for endurance and resistance training. Arch Phys Med Rehabil 2011;92(10):1663-1668. doi:10.1016/j.apmr.2011.04.022.
- Lemay JF, Nadeau S. Standing balance assessment in ASIA D paraplegic and tetraplegic participants: concurrent validity of the Berg Balance Scale. Spinal Cord 2010;48(3):245-250. doi:10.1038/sc.2009.119.
- Bohannon RW. Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants. Age Ageing 1997;26(1):15-19.
- Fulk GD, He Y, Boyne P, Dunning K. Predicting home and community walking activity poststroke. Stroke 2017;48(2):406-411. doi:10.1161/STROKEAHA.116.015309.
- MacLellan MJ, Patla AE. Adaptations of walking pattern on a compliant surface to regulate dynamic stability. Exp Brain Res 2006;173(3):521-530. doi:10.1007/s00221-006-0399-5.
- Zijlstra W, Rutgers AWF, Hof AL, Van Weerden TW. Voluntary and involuntary adaptation of walking to temporal and spatial constraints. Gait Posture 1995;3(1):13-18. doi:10.1016/0966-6362(95)90804-2.
- Oberg T, Karsznia A, Oberg K. Basic gait parameters: reference data for normal subjects, 10-79 years of age. J Rehabil Res Dev 1993;30(2):210-223.
- Hausdorff JM. Gait dynamics, fractals and falls: finding meaning in the stride-to-stride fluctuations of human walking. Hum Mov Sci 2007;26(4):555-589. doi:10.1016/j.humov.2007.05.003.
- Laufer Y. Effect of age on characteristics of forward and backward gait at preferred and accelerated walking speed. J Gerontol A Biol Sci Med Sci 2005;60(5):627-632.
- Sun J, Walters M, Svensson N, Lloyd D. The influence of surface slope on human gait characteristics: a study of urban pedestrians walking on an inclined surface. Ergonomics 1996;39(4):677-692. doi:10.1080/00140139608964489.
- Corrigan R, McBurney H. Community ambulation: environmental impacts and assessment inadequacies. Disabil Rehabil 2008;30(19):1411-1419. doi:10.1080/09638280701654542.
- Nanninga CS, Meijering L, Postema K, Schönherr MC, Lettinga AT. Unpacking community mobility: a preliminary study into the embodied experiences of stroke survivors. Disabil Rehabil 2017:1-10. doi:10.1080/09638288.2017.1323031.
- Olmos LE, Freixes O, Gatti MA, et al. Comparison of gait performance on different environmental settings for patients with chronic spinal cord injury. Spinal Cord 2008;46(5):331-334. doi:10.1038/sj.sc.3102132.
Gravel image courtesy of www.freeimages.com
7 Responses to “The Role of Terrain on Gait Speed and Spatiotemporal Measures”
Stacy Harris
Mike,
Thank you! I could not have done this without your guidance and never-ending patience. I appreciate all you do!
Laurie,
Thank you so much for your kind words! I am so glad you will be able to apply these results to your practice. I don’t think I could have had a better advisor during my time at UNC; you are the best!
Laurie Ray
This capstone clearly reflects a tremendous amount of work, excellent work. I am impressed. Especially by the clarity of your write up! I could visualize the set up and your outcomes and discussion peaked my interest. I will use this to support the need for PTs in public schools to work throughout the campus!! Well done!!
Michael Lewek
Stacy
You did a nice job pulling this all together. You and Alan did a lot of work over the past year, recruiting, testing, analyzing data, and writing. All good outcomes in the end.
Well done.
Stacy Harris
Hi Maddie!
Thank you so much for your kind response! I really like your suggestion of adding an asterisk to identify the significant results. I noticed that you did that for your presentation and I thought it was a great idea. With regard to the participants and their reactions during the outdoor terrains, the terrain that almost everyone commented on was going downhill on the gravel. Because of that, I anticipated it would be the terrain with the most change in the gait parameters, when the one that elicited the most change was usually the uphill gravel. It’s interesting that you asked that, because Alan compared their balance confidence with their performance and did not find a relationship. So, from an informal standpoint we saw that their confidence did not have an effect on their performance prior to getting that result from the data analysis. Finally, since all of the calculations for gait speed, step length, and cadence were completed after the fact, we didn’t have the chance to share the results directly with the participants. However, some asked after their trial what we were looking for and that led to some interesting discussions about what we expected the results to be and how they thought they did on the course.
Thanks again!
Stacy
Maddie Wygand
Hi Stacy!
You did a fantastic job with this project and your presentation at the CRC! As we discussed after your presentation, our research projects looked at similar outcome measures but in very different patient populations and scenarios. I think you did a great job with writing each section of this manuscript. The charts are very helpful for visualizing your findings. One additional thing that may be helpful with your charts is to add some type of indication (i.e. an asterisk, significance lines, etc.) to the conditions that had significant change so that the reader does not have to refer back and forth between the chart and written results.
The only question I had after reading your result is the same one that Ellie already asked about the effect of fatigue during the outdoor trial since it appears it was completed last and much longer distance than the level ground trial. It will be very interesting to see if you find anything when you run further analysis to assess for this factor.
Although I understand this is not part of your research question, I was curious if participants gave you any subjective response to the difference from level ground to uneven terrain? Did they feel confident? Find it more challenging? Feel unsteady? Were they surprised that their gait speed, step length, and/or cadence changed?
Overall, I love this research project and think this is valuable information when returning someone to the community safely!
Stacy Harris
Hi Ellie!
Thank you for your comments! Actually, we only had time for one trial of the 10 Meter Walk Test in the clinic. We were coordinating with the therapists around their treatment time and often the walking on the outdoor course was acceptable during treatment because it was being introduced into their plan of care on that day, so we were just observing (the therapists were aware of the path we wanted to take the patients on, we would give initial instructions, but they would walk with the patient for guarding purposes). You are correct that the outdoor course transitioned from one terrain to another without breaks. As a side note, we accounted for the transition by placing markers after the terrain began and before it ended to limit the risk of the transition skewing the results.
The purpose of doing two loops in opposite directions was mainly so that we could observe gait going downhill on the gravel and then going uphill on the gravel when going the opposite direction. This is anecdotal, but I believe in part due to our restriction of contact guard assistance or less, most participants were mobile enough that they did not need to rest between loops, but we did give all of them the option. Since the only terrain from the second loop included in the data analysis in my capstone was the uphill gravel (and the rest of the terrains had no slope), we did not address the potential for fatigue within my capstone project. In fact, one of the final terrains in the first loop was the small pavers, on which we saw no significant results for change in gait speed, step length, or cadence. So I don’t believe fatigue to be an issue during the first loop. However, we plan to run additional analysis prior to submitting a more complete draft for publication, so I will be interested to see if any differences in gait occurred on any of the terrains during the second loop where we did not receive significant results for the first loop. I hope this helps to clarify your questions!
Stacy
Elinor Rubin
Hi Stacy,
I am so impressed by all of the work you did in assisting with this research study. I especially benefited from your inclusion of graphical representation of study results. As a visual learner, they added tremendous value in helping me better understand your results.
You make a good point about some of the participants having previously completed the outdoor course and, as a result, may have performed better than those participants for whom this was their first time on the outdoor course. As part of the outdoor course data collection, you mentioned that participants were allowed to take a 5-minute rest break between the two loops. I am curious if there was a reason why you only completed 2 trials on the outdoor course on uneven terrains, as I am assuming you completed 3 trials for the timed 10-Meter Walk Test.
By your mention of the 5-minute rest break between loops, I also assume that participants did not stop between the different terrains while being timed on the outdoor course. It seems like by the final terrain-types that cadence and/or step length might also have been impacted by participant fatigue. Was having participants complete the outdoor course in reverse on the second trial an attempt to account for this and/or other potentially confounding factors?