Iliotibial Band Syndrome in Runners
Will Harrison, SPT
Background
My personal interest in the treatment of running injuries comes from dealing with numerous different injuries of my own since running cross country in high school. Furthermore, on my first clinical rotation at an outpatient orthopedic clinic after my first year of the DPT program, I saw several patients who complained of running injuries but I did not feel very confident in treating them effectively. Therefore, my personal interest in the topic along with the desire to expand my clinical knowledge and competence in evaluating and treating running injuries led to this project. While I have never personally dealt with Iliotibial Band Syndrome (ITBS), I have spoken with friends and colleagues who have had it, and I felt that this would be a particularly good topic to delve into.
Overview and Purpose
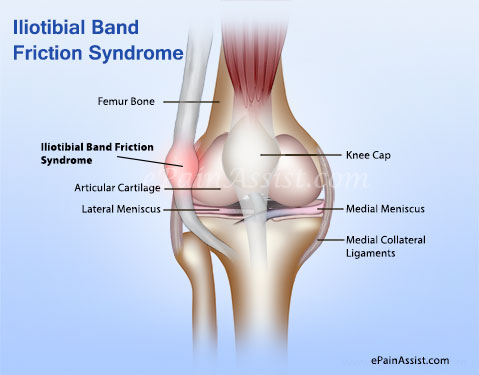
This topic is important to address because as clinicians, physical therapists are very likely to encounter patients in the clinic with sports and running injuries. In the United States, as many as 40 million people run regularly and over half of runners report some type of injury each year, mostly due to overuse.1 ITBS is an overuse injury of the lateral knee, and typically presents with insidious onset in runners.2 ITBS is the second most common cause of all knee pain and the most common cause of lateral knee pain in runners.3,4 The most characteristic description of ITBS is a sharp, piercing pain on the lateral aspect of the knee, over the lateral femoral condyle.
Personally, I have a broad range of clinical interests, but in the fall of 2016 I took the Advanced Orthopedic elective course, taught by Mike Gross, and also completed the Certified Strength and Conditioning Specialist (CSCS) independent study with Jon Hacke. Through these courses and prior classwork, I have developed a passion for working with the athletic population.
While ITBS is covered in the curriculum, I designed this Capstone Project to be incorporated as an optional module for PHYT 734 Musculoskeletal II-PT Intervention which students take in the fall semester of their 2nd year. I hope that this project provides students (and practicing clinicians) with additional insight into the topic of ITBS as well as greater confidence in evaluation and treatment of running injuries.
Products
I developed a VoiceThread Presentation, Iliotibial Band Syndrome in Runners Presentation, as well as an ITB Syndrome Evidence Table and ITB Syndrome Quick Reference Guide as part of this learning module. If you watch the VoiceThread, please take a couple minutes to also complete the ITB Syndrome Feedback Form so that I can continue to improve this learning module. In preparation for making this VoiceThread presentation, I wrote a brief paper, Application of Presentation Guidelines, that explains how I applied several concepts to ensure that the presentation is engaging and viewer friendly.
Reflection and Self-Assessment
Overall, I am satisfied with the quality of my capstone project. Based on the feedback that I received from my capstone committee, I expanded the evidence table and made several minor edits to both the presentation and quick reference guide. I feel that the project meets the learning objectives for the audience and will be a valuable resource to 2nd year students and practicing clinicians who wish to learn more about the topic of ITBS in runners.
Throughout the process of creating this presentation and the companion materials, I have learned several important things. First of all, I have learned a great deal about running injuries and I feel much more competent and confident in applying my clinical skills to the athletic population. I also feel more confident that I can take on the task of learning new and unfamiliar material and distilling it to the key points that would be most important for physical therapists. However, the differential diagnosis remains the greatest challenge for me, but I feel that as I gain experience I will become more proficient with my evaluation and assessment. Finally, I was able to learn how to use and apply the VoiceThread software to make an effective presentation. This has been an excellent experience for me, and I hope that others will find some benefit from my project as well.
Acknowledgements
I would like to sincerely thank my capstone committee advisor, Mike Gross, PT, PhD, FAPTA, for his assistance all along the way in helping me select an appropriate capstone topic and for providing valuable feedback regarding my presentation, evidence table, and quick reference guide. I would also like to thank my other committee members, Jon Hacke PT, DPT, MA, OCS, and Janet Hager, PT for their invaluable feedback, suggestions, and support. In particular, Jon was extremely helpful as I tried to ensure that the content of the material was appropriate for both 2nd year students and practicing clinicians. Janet’s feedback was vital as both a PT and a long-time runner who has dealt with ITB Syndrome in the past. This project would not have been possible without the support of my entire committee.
References
- Callahan L, Fields K, Grayzel J. Overview of Running Injuries of the Lower Extremity. UpToDate. http://www.uptodate.com/contents/overview-of-running-injuries-of-the-lower-extremity. Published 2016. Accessed January 22, 2017.
- Louw M, Deary C. The biomechanical variables involved in the aetiology of iliotibial band syndrome in distance runners – A systematic review of the literature. Phys Ther Sport. 2014;15(1):64-75. doi:10.1016/j.ptsp.2013.07.002.
- Baker RL, Fredericson M. Iliotibial Band Syndrome in Runners. Biomechanical Implications and Exercise Interventions. Phys Med Rehabil Clin N Am. 2016;27(1):53-77. doi:10.1016/j.pmr.2015.08.001.
- Aderem J, Louw QA. Biomechanical risk factors associated with iliotibial band syndrome in runners: a systematic review. BMC Musculoskelet Disord. 2015;16:1-16. doi:10.1186/s12891-015-0808-7.
Image from: https://www.epainassist.com/sports-injuries/knee-injuries/it-band-syndrome-or-iliotibial-band-friction-syndrome
5 Responses to “Iliotibial Band Syndrome in Runners”
Kristen Ignaszewski
Will,
I think the topic of iliotibial band syndrome in runners was an excellent choice for your capstone project, as it seems to be a prevalent overuse issue in this patient population. Going into an outpatient orthopedic setting after graduation, I am sure I will see patients presenting with ITBS. Your VoiceThread was informative and I appreciated that you went above and beyond by also creating an evidence table and a quick reference guide. The review of anatomy and biomechanics, risk factors, and section on differential diagnosis will be particularly beneficial in conjunction with the evaluation and assessment information. I know I will be looking back at your reference guide when a new running patient comes into the clinic! Great job on your capstone project!!
Thanks, Kristen!
-Will
anne hammonds
Hi Will,
You have done a great job with your Capstone site. I enjoyed your voicethread and found it to be concise and informative in presenting the most current information on ITB. I am sure this will be a great resource for the second year students if they enroll in the Advance Orthopedics course with Dr Gross and a great refresher for alumni that may not have been practicing in orthopedics in a while.
In my previous job at a private OPPT clinic, we would regularly see patients with knee pain related to running on the roads > trails. (Your differential diagnosis slide would have been very helpful to me then). My own empirical findings at that time led me to obvious issues with these patients: 1) hip abduction weakness 2) gait pattern (specifically heel strike).
My patients that ran on the roads were primarily moving in a sagittal plane and therefore as the abductors fagitued, they would lose their form and develop lateral knee pain. My thinking was that the trail runners were constantly hopping over logs, rocks and roots and strengthening their hip muscles rather than overusing a specific muscle.
Changing the gait pattern from heel strike to mid/fore foot strike increased their cadence (described in your research) and decreased the amount of time the knee was in near-full extension (heel strike) transitioning to knee flexion (at stance phase & close to 30* flexion).
I am curious if any of your research discussed how the ‘barefoot running’ craze has altered the incidence of IT band pain.
You’ve done a very nice job with your Capstone project that will be referenced for years to come. Congratulations.
Hi Anne,
Thanks for visiting my site! I am so appreciative to hear your thoughts since you are a practicing clinician and have treated patients with ITBS in your clinic. Unfortunately, I found very little information regarding the barefoot running craze, but I agree with you that it would be interesting to see what the findings would be for this. I know that barefoot runners tend to have an increased cadence and also tend to strike with either the midfoot or forefoot, so I’m not sure whether or not ITBS would be an issue. Barefoot running certainly opens a whole other can of worms though! Thanks again for your thoughts, I really appreciate it!
Will
Jessica Reynolds
Hi Will,
Excellent presentation! As someone who has experienced ITB issues from running, I really appreciated your rationale behind the potential causes and treatments. Interestingly, I noted that reduced hip abductor strength was a potential risk factor from your presentation. This seems to be true in my case after many years of on and off ITB syndrome. Since I began to focus on hip abductor strength several years ago, I haven’t had an ITB problem. Also, I hadn’t previously heard of the friction and impingement vs. compression argument, and it was helpful to consider both of these perspectives and the theories behind them in your presentation.
Questions:
1.) You noted that the patients should start with open chain exercises when strengthening, and then move on to closed chained. Do you know the rationale for this?
2.) What was the rationale in increasing cadence for the case study to 176 steps per minute? Was that supposed to help tie in with midfoot striking, or for another reason? (slide 35)
A few other notes:
Your organization and pacing was excellent, and it was thoughtful to include a nice little break to help participants regain focus. Your use of visual aids on the slides was also excellent. It really helped me to focus and understand the content. I thought that the case study was a great way to bring everything together.
Great work! This is an excellent resource that many students and PTs can benefit from, and I’m sure that their future patients will be grateful.
Hi Jess,
Thanks for visiting my site! I’ll do my best to answer your questions:
1. The article by Fredericson et al (referenced in the VoiceThread) was the main article that promoted beginning with open-chain and then progressing to closed-chain, but the authors did not provide a detailed rationale. However, based on my understanding of the rehab process and from reading some other articles on the topic, there are a couple main reasons. First of all, if there is specific weakness in one component of the kinetic chain, then that one component needs to be isolated and strengthened before it is added back into the chain. Otherwise, you may end up with a situation where you have continued faulty mechanics or other muscle groups compensating for weakness elsewhere. Second, since running is a closed-chain activity in stance phase (and remember, pain is usually in stance phase with ITBS), then this should be the last phase of strengthening/recovery before the return-to-running phase. However, every patient is different, and severity of symptoms will certainly dictate the exercise progression.
2. Regarding running cadence- The authors from the Allen et al study cited another research article by Heiderscheidt et al in which the authors found that when runners increase their cadence by 5-10%, it results in decreased heel strike, decreased step length, decreased braking impulse, and decreased vertical excursion. So, by instructing someone to run with a greater cadence, you can essentially alter that person’s foot-strike pattern and decrease the overall ground reaction forces experienced during stance phase. An easy way to do this is by giving a patient a metronome which they can listen to while they are running until the new gait pattern becomes second nature. Thinking back to the principles of motor learning, this gives the runner an external focus rather than an internal focus, and may make it easier for the PT to actually implement the intervention.
Thanks again, and I hope that helps!
Will
Anthony Pastore
Hey Will,
Awesome job! As a runner and as someone who hopes to specialize in the treatment of runners in my future practice, this topic is something that I have a lot of interest in. I think that your presentation is a great resource for both second year PT students and clinicians who may not be familiar with the examination, evaluation, and treatment of individuals who may be suffering from ITB syndrome. You seem to have a good handle on presentation skills and presenting information in an easily digestible manner. The evidence table and quick reference guide that you produced are two pieces of material that I could definitely see myself utilizing as I start to gain more exposure to the treatment of this population, so excellent job there as well! I would agree with Colleen’s question above. I wrote about patellofemoral pain syndrome in runners for Mike’s Advanced Orthopedic class, and orthotics is an intervention that was discussed pretty heavily. Is this an intervention that has been studied much for ITB syndrome? Also, I know there is some controversy about the ability to stretch the ITB as well as myofascial release, foam rolling, etc. Did you get a sense of the efficacy of these interventions during your research?
Again, great job! Good luck going into your final rotation. I hope you get the opportunity to apply some of this information into practice.
Hi Anthony,
Thanks for visiting my site! To answer your first question regarding orthotics/footwear, see my response to Colleen above. As far as your second question regarding stretching and/or foam rolling for the ITB: yes, I definitely found some information but not a lot of specific findings from the research (more just general clinician recommendations). Several of the articles that I referenced in the VoiceThread (specifically the Baker article, Allen article, and the Strauss article) have some nice specific suggestions for stretching and foam rolling with pictures. So, for more detailed information about that topic, you could check out those resources. Generally however, stretching and foam rolling are advocated by many clinicians for stretching and myofascial release of the ITB and other hip musculature. I hope that answers your questions, and thanks again for checking out my page. Good luck on your final rotation as well!
Will
Colleen Johnson
Will,
Great presentation! As a clinician who sees ITBS frequently, your VoiceThread gave me a great “refresher” on anatomy and the pathophysiology as well as ideas for exercises. I was wondering, you mention a possible biomechanical risk factor being forefoot varus and/or foot pronation; in your research, did you come across evidence for the benefits of orthotics or specific footwear for correction? If so, do you think this should be implemented early in the treatment or wait to see if the symptoms improve with the other interventions first? Again, wonderful job!
Colleen
Thanks, Colleen!
So, I was actually surprised by how little specific information I could find regarding recommendations and benefits of orthotics or other specific footwear. I had the same initial thought as you, and would have expected more authors to address this topic in their research papers. However, after speaking with my advisor (Mike Gross) and my other capstone committee members, we agreed that footwear is definitely an important consideration. As to your question about how and when to implement that intervention, I guess it just depends on the patient and your own clinical judgment, because right now the research is sparse on the topic. I hope that helps- thanks again for visiting my site!
Best,
Will